Division of Cardiology, Department of Internal Medicine, University of Texas Southwestern Medical Center, Dallas (A.P., S.S.).
Department of Cardiology, Texas Heart Institute, Houston (M.W.S.).
Circulation. 2022 Jul 12;146(2):80-90. doi: 10.1161/CIRCULATIONAHA.122.059983. Epub 2022 May 26.
Supervised aerobic exercise training (ET) is recommended for stable outpatients with heart failure (HF) with reduced ejection fraction (HFrEF). Frailty, a syndrome characterized by increased vulnerability and decreased physiologic reserve, is common in patients with HFrEF and associated with a higher risk of adverse outcomes. The effect modification of baseline frailty on the efficacy of aerobic ET in HFrEF is not known.
Stable outpatients with HFrEF randomized to aerobic ET versus usual care in the HF-ACTION (Heart Failure: A Controlled Trial Investigating Outcomes of Exercise Training) trial were included. Baseline frailty was estimated using the Rockwood frailty index (FI), a deficit accumulation-based model of frailty assessment; participants with FI scores >0.21 were identified as frail. Multivariable Cox proportional hazard models with multiplicative interaction terms (frailty × treatment arm) were constructed to evaluate whether frailty modified the treatment effect of aerobic ET on the primary composite end point (all-cause hospitalization or mortality), secondary end points (composite of cardiovascular death or cardiovascular hospitalization, and cardiovascular death or HF hospitalization), and Kansas City Cardiomyopathy Questionnaire score. Separate models were constructed for continuous (FI) and categorical (frail versus not frail) measures of frailty.
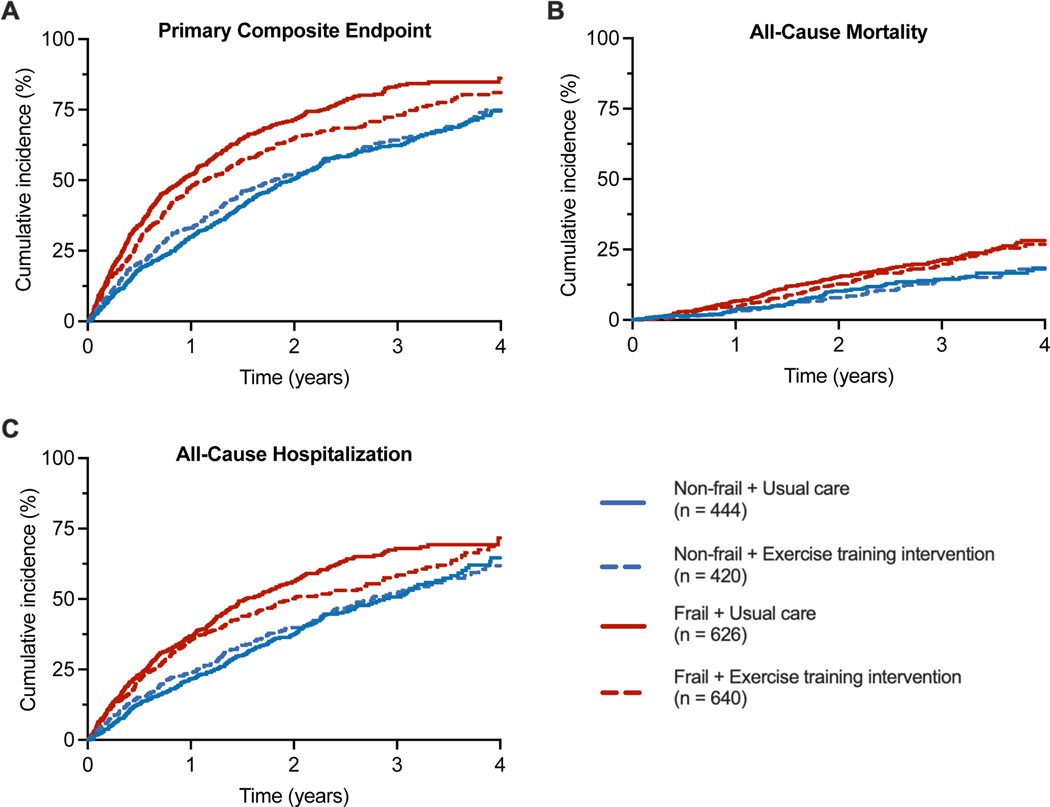
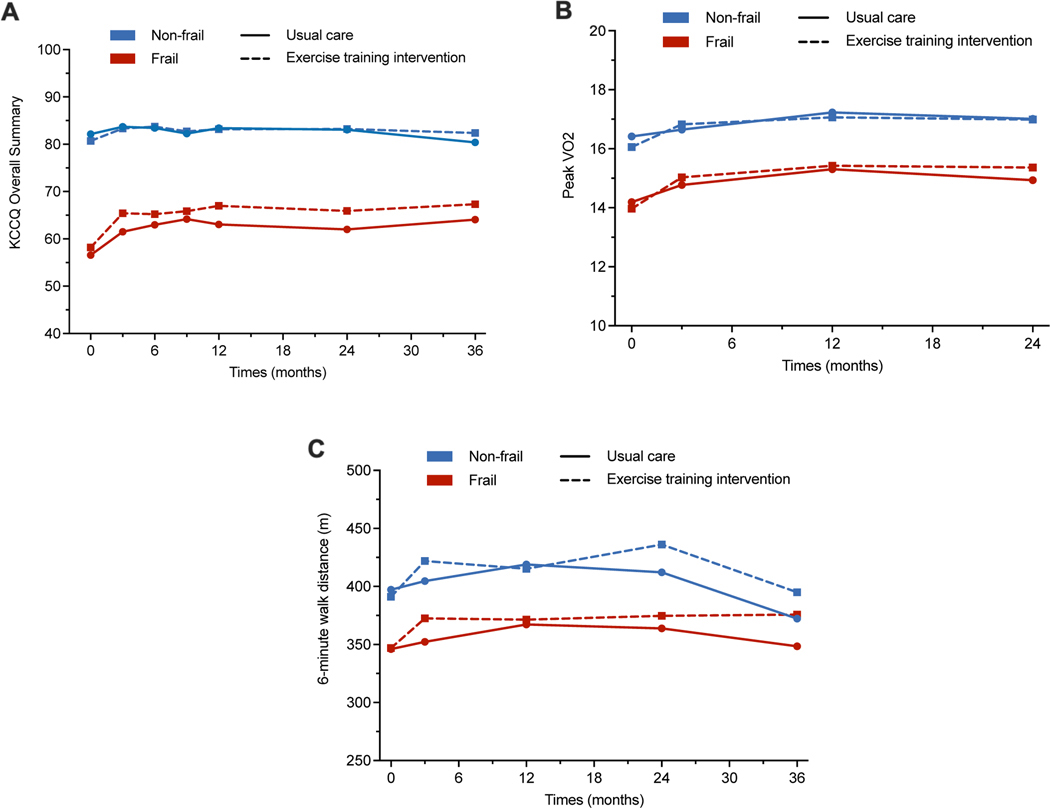
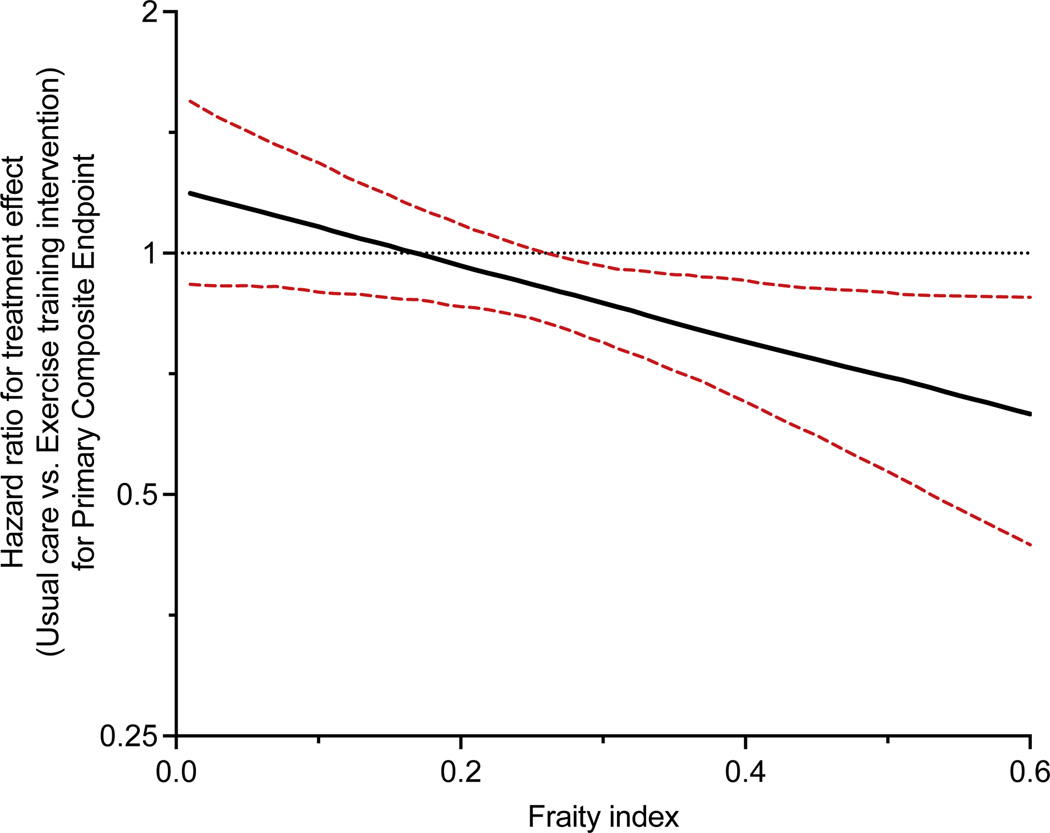
Among 2130 study participants (age, 59±13 years; 28% women), 1266 (59%) were characterized as frail (FI>0.21). Baseline frailty burden significantly modified the treatment effect of aerobic ET ( interaction: FI × treatment arm=0.02; frail status [frail versus nonfrail] × treatment arm=0.04) with a lower risk of primary end point in frail (hazard ratio [HR], 0.83 [95% CI, 0.72-0.95]) but not nonfrail (HR, 1.04 [95% CI, 0.87-1.25]) participants. The favorable effect of aerobic ET among frail participants was driven by a significant reduction in the risk of all-cause hospitalization (HR, 0.84 [95% CI, 0.72-0.99]). The treatment effect of aerobic ET on all-cause mortality and other secondary endpoints was not different between frail and nonfrail patients ( interaction>0.1 for each). Aerobic ET was associated with a nominally greater improvement in Kansas City Cardiomyopathy Questionnaire scores at 3 months among frail versus nonfrail participants without a significant treatment interaction by frailty status ( interaction>0.2).
Among patients with chronic stable HFrEF, baseline frailty modified the treatment effect of aerobic ET with a greater reduction in the risk of all-cause hospitalization but not mortality.
对于射血分数降低的心力衰竭(HFrEF)稳定门诊患者,推荐进行有监督的有氧运动训练(ET)。衰弱是一种以易损性增加和生理储备减少为特征的综合征,在 HFrEF 患者中很常见,与不良结局的风险增加相关。基线衰弱对 HFrEF 中有氧运动 ET 疗效的影响修饰尚不清楚。
HF-ACTION(心力衰竭:一项评估运动训练结果的对照试验)试验中,将随机分配至有氧运动 ET 与常规治疗的 HFrEF 稳定门诊患者纳入研究。使用 Rockwood 衰弱指数(FI)估计基线衰弱情况,FI 是一种基于缺陷积累的衰弱评估模型;FI 评分>0.21 的患者被认定为衰弱。构建多变量 Cox 比例风险模型,包含乘法交互项(衰弱×治疗臂),以评估衰弱是否修饰了有氧运动 ET 对主要复合终点(全因住院或死亡率)、次要终点(心血管死亡或心血管住院复合终点,以及心血管死亡或心力衰竭住院复合终点)和堪萨斯城心肌病问卷评分的治疗效果。分别为连续(FI)和分类(衰弱与非衰弱)衰弱测量值构建了单独的模型。
在 2130 名研究参与者中(年龄 59±13 岁;28%为女性),1266 名(59%)患者表现出衰弱(FI>0.21)。基线衰弱负担显著修饰了有氧运动 ET 的治疗效果(交互:FI×治疗臂=0.02;衰弱状态[衰弱与非衰弱]×治疗臂=0.04),衰弱患者的主要终点风险降低(风险比[HR],0.83[95%CI,0.72-0.95]),而非衰弱患者则无此风险(HR,1.04[95%CI,0.87-1.25])。在衰弱患者中,有氧运动 ET 的有益效果是由于全因住院风险的显著降低(HR,0.84[95%CI,0.72-0.99])。在衰弱和非衰弱患者中,有氧运动 ET 对全因死亡率和其他次要终点的治疗效果无差异(交互>0.1 )。与非衰弱参与者相比,在衰弱参与者中,有氧运动 ET 治疗 3 个月后堪萨斯城心肌病问卷评分的改善具有显著的改善趋势,但按衰弱状态的治疗交互作用不明显(交互>0.2)。
在慢性稳定的 HFrEF 患者中,基线衰弱修饰了有氧运动 ET 的治疗效果,全因住院风险降低,但死亡率无变化。