Julius Centre for Health Sciences and Primary Care, University Medical Centre Utrecht, Utrecht, the Netherlands.
Department of General Practice and Elderly Care Medicine, VU University Medical Centre, Amsterdam, the Netherlands.
United European Gastroenterol J. 2020 Jun;8(5):607-620. doi: 10.1177/2050640620917804. Epub 2020 Apr 6.
An efficient diagnostic pathway and early stage diagnosis for cancer patients is widely pursued. This study aims to chart the duration of the diagnostic pathway for patients with symptomatic oesophageal and gastric cancer, to identify factors associated with long duration and to assess the association of duration with tumour stage at diagnosis.
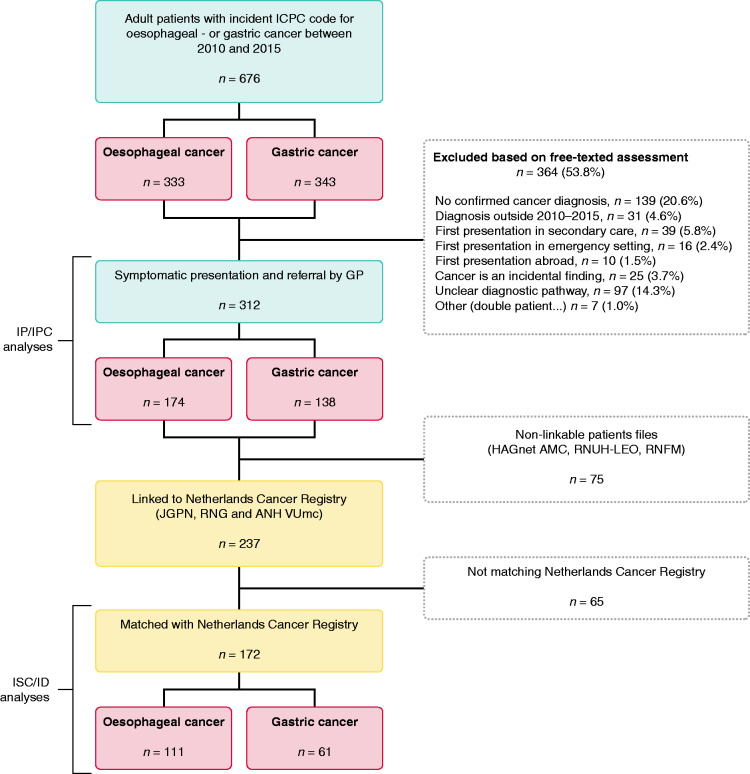
This was a retrospective cohort study, using electronic health records of six routine primary care databases covering about 640,000 patients, partly linked to the Netherlands Cancer Registry. Symptomatic patients with oesophageal and gastric cancer (2010-2015) that presented in primary care were included. Duration of four diagnostic intervals was determined: patient interval; first symptoms to primary care consultation, primary care interval; consultation to referral, secondary care interval; referral to diagnosis, and the diagnostic interval; consultation to diagnosis. Characteristics associated with 'long duration' (≥P75 duration) were assessed using log-binomial regression. Median durations were stratified for tumour stages.
Among 312 symptomatic patients with upper gastrointestinal cancer, median durations were: patient interval: 29 days (interquartile interval 15-73), primary care interval: 12 days (interquartile interval 1-43), secondary care interval: 13 days (interquartile interval 6-29) and diagnostic interval: 31 days (11-74). Patient interval duration was comparable for patients with and without alarm symptoms. Absence of cancer-specific alarm symptoms was associated with 'long duration' of primary care interval and secondary care interval: relative risk 5.0 (95% confidence interval 2.7-9.1) and 2.1 (95% confidence interval 1.3-3.7), respectively. Median diagnostic interval duration for local stage disease was 51 days (interquartile interval 13-135) versus 27 days (interquartile interval 11-71) for advanced stage ( = 0.07).
In the diagnostic pathway of upper gastrointestinal cancers, the longest interval is the patient interval. Reducing time to diagnosis may be achieved by improving patients' awareness of alarm symptoms and by diagnostic strategies which better identify cancer patients despite low suspicion.
人们广泛追求为癌症患者提供高效的诊断途径和早期诊断。本研究旨在绘制有症状的食管癌和胃癌患者的诊断途径持续时间图,确定与长时间相关的因素,并评估诊断持续时间与诊断时肿瘤分期的相关性。
这是一项回顾性队列研究,使用六个常规初级保健数据库的电子健康记录,这些数据库涵盖了约 640000 名患者,部分与荷兰癌症登记处相关联。纳入了在初级保健中出现有症状的食管癌和胃癌(2010-2015 年)的患者。确定了四个诊断间隔的持续时间:患者间隔;从首次出现症状到初级保健就诊,初级保健间隔;就诊到转诊,二级保健间隔;转诊到诊断,以及诊断间隔;就诊到诊断。使用对数二项式回归评估与“长时间”(≥P75 持续时间)相关的特征。根据肿瘤分期对中位数持续时间进行分层。
在 312 名有上消化道癌症症状的患者中,中位持续时间为:患者间隔:29 天(四分位间距 15-73),初级保健间隔:12 天(四分位间距 1-43),二级保健间隔:13 天(四分位间距 6-29)和诊断间隔:31 天(11-74)。有和没有警报症状的患者的患者间隔持续时间相当。缺乏癌症特异性警报症状与初级保健间隔和二级保健间隔的“长时间”相关:相对风险分别为 5.0(95%置信区间 2.7-9.1)和 2.1(95%置信区间 1.3-3.7)。局部阶段疾病的中位诊断间隔持续时间为 51 天(四分位间距 13-135),而晚期疾病为 27 天(四分位间距 11-71)(=0.07)。
在上消化道癌症的诊断途径中,最长的间隔是患者间隔。通过提高患者对警报症状的认识并通过诊断策略来更好地识别癌症患者,尽管怀疑程度较低,但可以缩短诊断时间。