Center for Paediatrics and Adolescent Medicine, University Medical Center, Faculty of Medicine, University of Freiburg, Germany; Faculty of Public Health and Policy, London School of Hygiene & Tropical Medicine, United Kingdom.
Department of Infectious Disease Epidemiology, London School of Hygiene & Tropical Medicine, United Kingdom.
Vaccine. 2020 Apr 29;38(20):3627-3638. doi: 10.1016/j.vaccine.2020.03.040. Epub 2020 Apr 3.
Ethiopia is a priority country of Gavi, the Vaccine Alliance to improve vaccination coverage and equitable uptake. The Ethiopian National Expanded Programme on Immunisation (EPI) and the Global Vaccine Action Plan set coverage goals of 90% at national level and 80% at district level by 2020. This study analyses full vaccination coverage among children in Ethiopia and estimates the equity impact by socioeconomic, geographic, maternal and child characteristics based on the 2016 Ethiopia Demographic and Health Survey dataset.
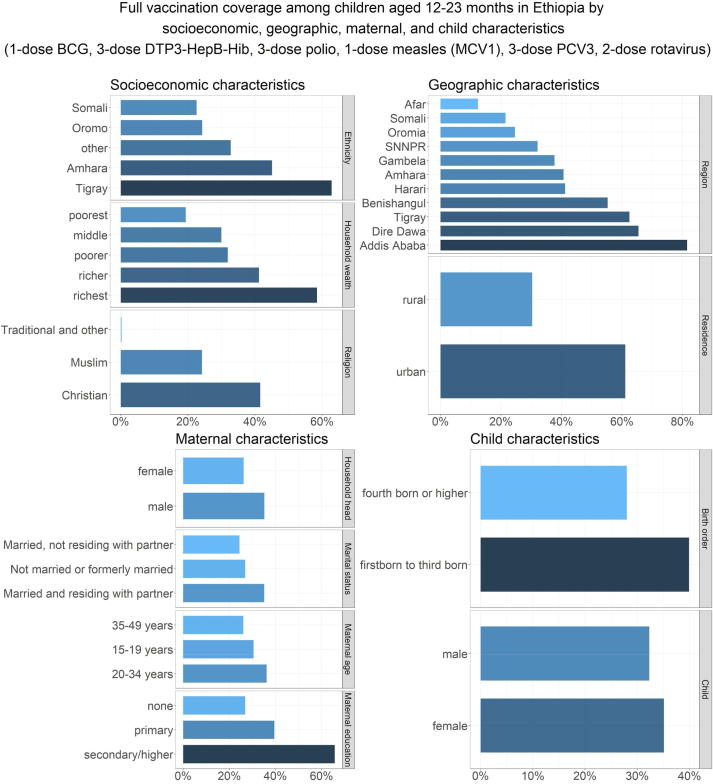
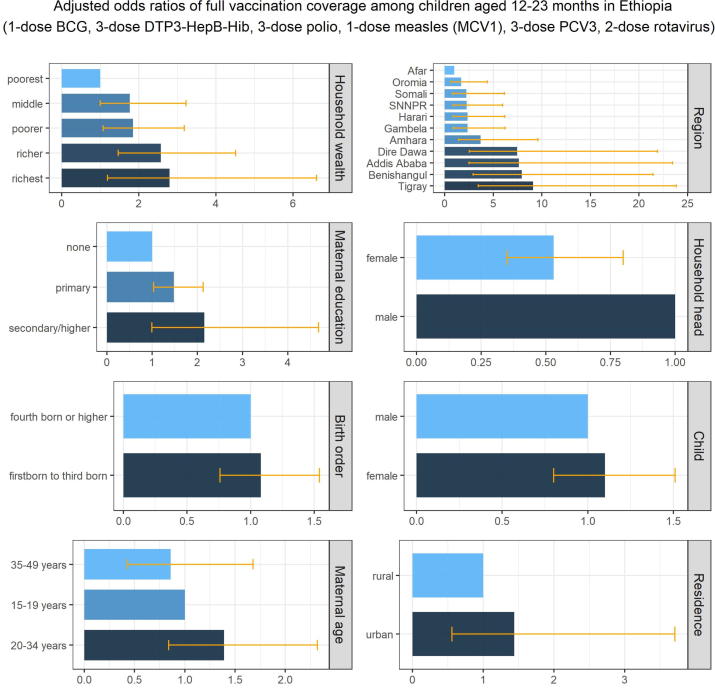
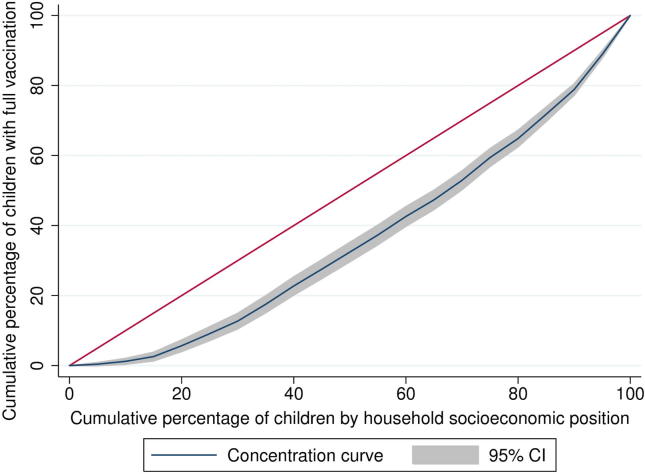
Full vaccination coverage (1-dose BCG, 3-dose DTP3-HepB-Hib, 3-dose polio, 1-dose measles (MCV1), 3-dose pneumococcal (PCV3), and 2-dose rotavirus vaccines) of 2,004 children aged 12-23 months was analysed. Mean coverage was disaggregated by socioeconomic (household wealth, religion, ethnicity), geographic (area of residence, region), maternal (maternal age at birth, maternal education, maternal marital status, sex of household head), and child (sex of child, birth order) characteristics. Concentration indices estimated wealth and education-related inequities, and multiple logistic regression assessed associations between full vaccination coverage and socioeconomic, geographic, maternal, and child characteristics.
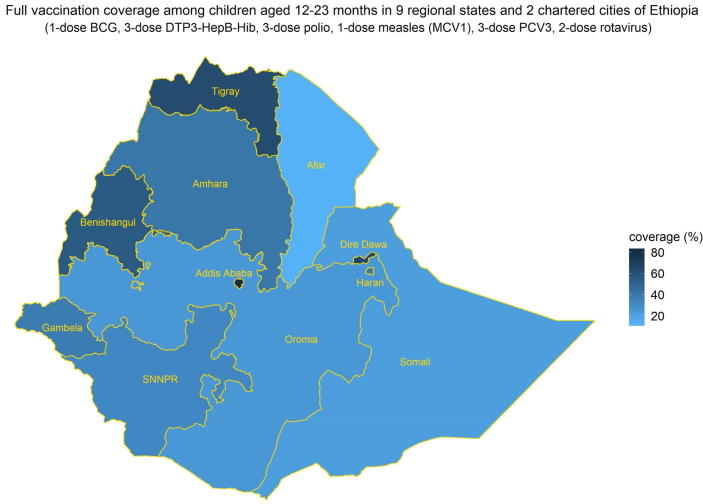
Full vaccination coverage was 33.3% [29.4-37.2] in 2016. Single vaccination coverage ranged from 49.1% [45.1-53.1] for PCV3 to 69.2% [65.5-72.8] for BCG. Wealth and maternal education related inequities were pronounced with concentration indices of 0.30 and 0.23 respectively. Children in Addis Ababa and Dire Dawa were seven times more likely to have full vaccination compared to children living in the Afar region. Children in female-headed households were 49% less likely to have full vaccination.
Vaccination coverage in Ethiopia has a pro-advantaged regressive distribution with respect to both household wealth and maternal education. Children from poorer households, rural regions of Afar and Somali, no maternal education, and female-headed households had lower full vaccination coverage. Targeted programmes to reach under-immunised children in these subpopulations will improve vaccination coverage and equity outcomes in Ethiopia.
埃塞俄比亚是疫苗联盟(Gavi)的重点国家,旨在提高疫苗接种覆盖率和公平性。埃塞俄比亚国家扩大免疫规划(EPI)和全球疫苗行动计划设定了到 2020 年全国覆盖率达到 90%、地区覆盖率达到 80%的目标。本研究基于 2016 年埃塞俄比亚人口与健康调查数据集,分析了埃塞俄比亚儿童的完全疫苗接种覆盖率,并根据社会经济、地理、母婴特征评估了公平性影响。
对 2004 名 12-23 个月龄儿童的完全疫苗接种覆盖率(1 剂卡介苗、3 剂 DTP3-乙肝-Hib、3 剂脊髓灰质炎、1 剂麻疹(MCV1)、3 剂肺炎球菌(PCV3)和 2 剂轮状病毒疫苗)进行了分析。按社会经济(家庭财富、宗教、族裔)、地理(居住地区、区域)、母婴(母婴出生年龄、母婴教育程度、母婴婚姻状况、家庭户主性别)和儿童(儿童性别、出生顺序)特征对平均覆盖率进行了细分。集中指数估计了财富和教育相关的不平等,多因素逻辑回归评估了完全疫苗接种覆盖率与社会经济、地理、母婴和儿童特征之间的关联。
2016 年,完全疫苗接种覆盖率为 33.3%[29.4-37.2]。单剂疫苗接种覆盖率从 PCV3 的 49.1%[45.1-53.1]到 BCG 的 69.2%[65.5-72.8]不等。财富和母婴教育的不平等程度明显,集中指数分别为 0.30 和 0.23。与居住在阿法尔地区的儿童相比,亚的斯亚贝巴和 Dire Dawa 的儿童完全接种疫苗的可能性高出七倍。女童当家的家庭儿童完全接种疫苗的可能性要低 49%。
埃塞俄比亚的疫苗接种覆盖率呈有利于优势人群的倒退分布,这与家庭财富和母婴教育都有关。来自较贫困家庭、阿法尔和索马里农村地区、没有母婴教育和女童当家的家庭的儿童完全接种疫苗的覆盖率较低。针对这些亚人群的目标计划将提高埃塞俄比亚的疫苗接种覆盖率和公平性结果。