Omar Michael Brandon, Kogler William, Maharaj Satish, Aung Win
1Department of Medicine, University of Florida College of Medicine-Jacksonville, Jacksonville, USA.
2Division of Medical Oncology and Hematology, University of Louisville, Louisville, USA.
Clin Hypertens. 2020 Apr 1;26:6. doi: 10.1186/s40885-020-00140-4. eCollection 2020.
Renal artery stenosis is a notorious cause of secondary hypertension which classically presents as chronic refractory hypertension, recurrent flash pulmonary edema or renal insufficiency after initiation of an angiotensin converting enzyme inhibitor. Rarely, there have been reported cases of pregnant patients presenting with new onset or superimposed preeclampsia secondary to renovascular hypertension. In this subset of patients, renovascular hypertension carries significantly higher risks including obstetric, fetal and medical emergencies and death. Prompt treatment is required. However, the teratogenic risks of radiological investigations and antihypertensive medications limit diagnostic and management options thus posing quite a dilemma.
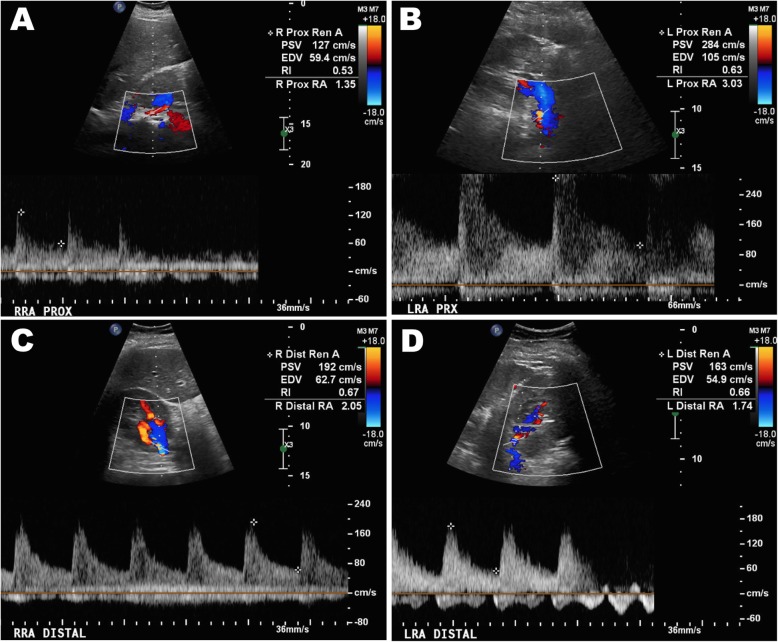
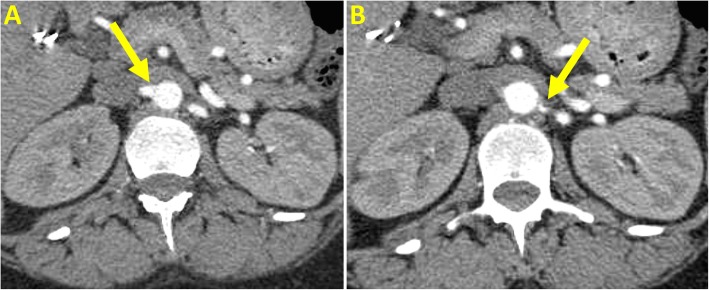
A 38-year-old female, at 33 weeks of gestation, was hospitalized for preeclampsia with severe features. A viable neonate had been expeditiously delivered yet the patient's post-partum blood pressures remained severely elevated despite multi-class anti-hypertensive therapy. Renal artery dopplers revealed greater than 60% stenosis of the proximal left renal artery and at least 60% stenosis of the right renal artery. Renal angiography showed 50% stenosis of the left proximal renal artery for which balloon angioplasty and stenting was performed. The right renal artery demonstrated less than 50% stenosis with an insignificant hemodynamic gradient, thus was not stented. Following revascularization, the patient's blood pressure improved within 48 h, on dual oral antihypertensive therapy.
Preeclampsia that is refractory to multi-drug antihypertensive therapy should raise suspicion for renal artery stenosis. Suspected patients can be screened safely with Doppler ultrasonography which can be then followed by angiography. Even if renal artery stenosis does not seem severe, early renal revascularization may be considered in patients with severe preeclampsia who do not respond to antihypertensive management.
肾动脉狭窄是继发性高血压的一个常见病因,典型表现为慢性难治性高血压、复发性急性肺水肿或在开始使用血管紧张素转换酶抑制剂后出现肾功能不全。很少有报道称,孕妇会出现新发或叠加的子痫前期,继发于肾血管性高血压。在这部分患者中,肾血管性高血压带来的风险显著更高,包括产科、胎儿及医疗紧急情况和死亡。需要及时治疗。然而,放射学检查和抗高血压药物的致畸风险限制了诊断和管理选择,因此造成了相当大的困境。
一名38岁女性,孕33周,因重度子痫前期住院。已迅速分娩出一名存活新生儿,但尽管采用了多种抗高血压治疗,患者产后血压仍严重升高。肾动脉多普勒检查显示左肾动脉近端狭窄超过60%,右肾动脉狭窄至少60%。肾血管造影显示左肾动脉近端狭窄50%,为此进行了球囊血管成形术和支架置入术。右肾动脉狭窄小于50%,血流动力学梯度不显著,因此未进行支架置入。血管重建术后,患者在双重口服抗高血压治疗下,48小时内血压有所改善。
对多种药物抗高血压治疗无效的子痫前期应怀疑肾动脉狭窄。疑似患者可通过多普勒超声进行安全筛查,随后可进行血管造影。即使肾动脉狭窄似乎不严重,对于对抗高血压治疗无反应的重度子痫前期患者,也可考虑早期肾血管重建术。