Martin Sven, Thome Ulrich Herbert, Grunwald Martin, Mueller Stephanie Margarete
Haptic Research Lab, Paul Flechsig Institute for Brain Research, Leipzig University, Leipzig, Germany.
Department of Neonatology, University Hospital Leipzig, Leipzig, Germany.
Front Pediatr. 2020 Mar 17;8:102. doi: 10.3389/fped.2020.00102. eCollection 2020.
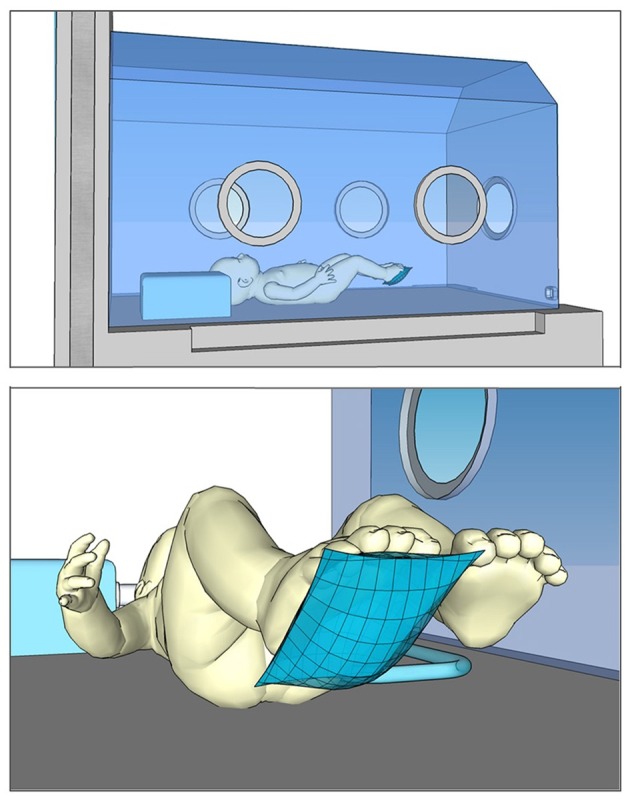
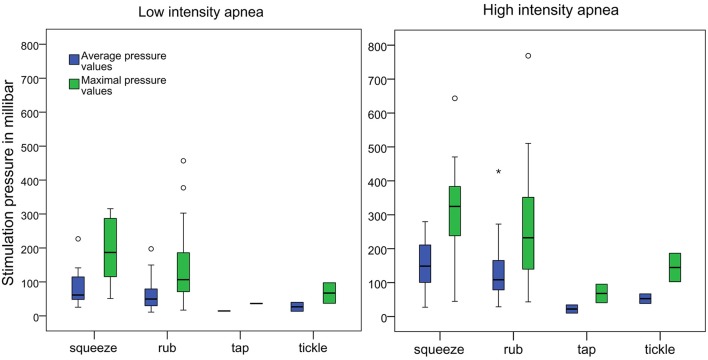
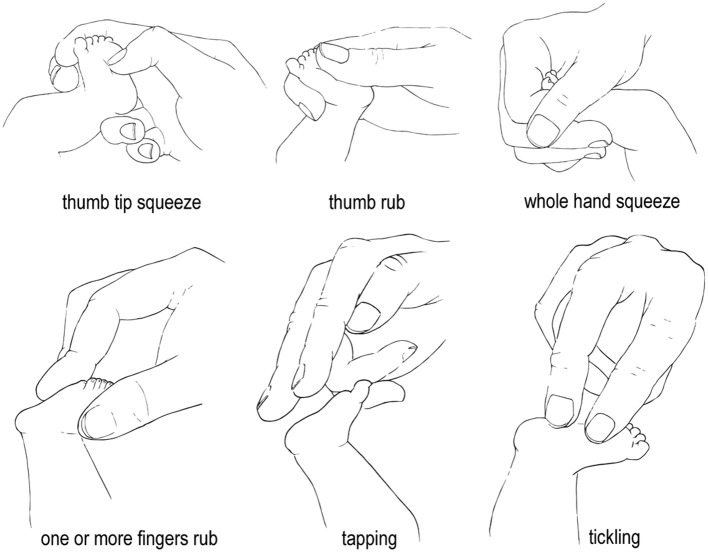
Even though tactile stimulation is common practice to terminate preterm apnea, the style and intensity of these interventions is not specified during theoretical or practical training and has never been clinically evaluated. The present study was designed to analyze the various modes of tactile stimulation used to terminate preterm apnea and measure the pressure intensity and frequency of these stimulations. A model with the size and weight of an actual preterm infant was equipped with sensor technology to measure stimulation pressure and frequency of tactile stimulation. Additionally a camera system was used to record hand positions and stimulation modes. Seventy medical staff members took part in the experiment. We found extreme between subjects differences in stimulation pressure that could not be explained by professional experience but, to a degree, depended on apnea intensity. Pressures ranged from 11.11 to 226.87 mbar during low intensity apnea and from 9.89 to 428.15 mbar during high intensity apnea. The majority of participants used rhythmic stimulation movements with a mean frequency of ~1 Hz. Different modes (rubbing, squeezing, tickling, and tapping) and finger positions were used. Medical staff members intuitively adjust their tactile stimulation pressure depending on the premature infants' apnea intensity. However, mean pressure values varied greatly between subjects, with similar pressure ranges for low and high intensity apnea. The question remains which pressure intensities are necessary or sufficient for the task. It is reasonable to assume that some stimulation types may be more effective in rapidly terminating an apneic event.
尽管触觉刺激是终止早产儿呼吸暂停的常用方法,但在理论或实践培训中,这些干预措施的方式和强度并未明确规定,也从未进行过临床评估。本研究旨在分析用于终止早产儿呼吸暂停的各种触觉刺激模式,并测量这些刺激的压力强度和频率。一个具有实际早产儿大小和重量的模型配备了传感器技术,以测量触觉刺激的压力和频率。此外,还使用了一个摄像系统来记录手部位置和刺激模式。70名医护人员参与了实验。我们发现,受试者之间的刺激压力存在极大差异,这无法用专业经验来解释,但在一定程度上取决于呼吸暂停的强度。在低强度呼吸暂停期间,压力范围为11.11至226.87毫巴,在高强度呼吸暂停期间,压力范围为9.89至428.15毫巴。大多数参与者使用频率约为1赫兹的有节奏的刺激动作。使用了不同的模式(摩擦、挤压、挠痒和轻拍)和手指位置。医护人员会根据早产儿的呼吸暂停强度直观地调整触觉刺激压力。然而,受试者之间的平均压力值差异很大,低强度和高强度呼吸暂停的压力范围相似。问题仍然是,对于这项任务,哪些压力强度是必要的或足够的。可以合理地假设,某些刺激类型可能在迅速终止呼吸暂停事件方面更有效。