Division of Medical Oncology, Department of Internal Medicine, Yonsei Cancer Center, Yonsei University College of Medicine, 50-1 Yonsei-ro, Seodaemun-gu, Seoul, 03722, South Korea.
Brain Korea 21 Plus Project for Medical Sciences, Yonsei University College of Medicine, Seoul, South Korea.
Trials. 2020 Apr 7;21(1):320. doi: 10.1186/s13063-020-04266-6.
Preoperative chemoradiotherapy (PCRT) followed by surgery and adjuvant chemotherapy is the current standard treatment for stage II/III rectal cancer. However, radiotherapy in the pelvic area is commonly associated with complications such as anastomotic leakage, sexual dysfunction, and fecal incontinence. Recently, the MERCURY study showed that preoperative high-resolution magnetic resonance imaging (MRI) helped to selectively avoid PCRT. It remains unclear whether PCRT is necessary in patients who can achieve a negative circumferential resection margin (CRM) with surgery alone and in patients with cTN or cTN without CRM involvement and lateral lymph node metastasis. This study aims to evaluate the efficacy of upfront radical surgery with total mesorectal excision (TME) followed by adjuvant chemotherapy with folinic acid (or leucovorin), fluorouracil, and oxaliplatin (FOLFOX) versus the current standard treatment in patients with surgically resectable, locally advanced rectal cancer.
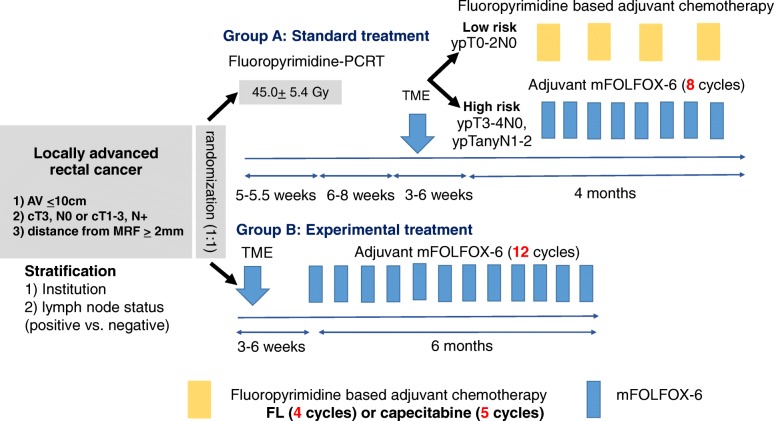
This study, named TME-FOLFOX, is a prospective, open-label, multicenter, phase II randomized trial. Patients with locally advanced rectal cancer will be randomized to receive PCRT followed by TME and adjuvant chemotherapy (arm A) or upfront radical surgery with TME followed by adjuvant FOLFOX chemotherapy (arm B). Clinical stage II/III rectal cancer without CRM involvement and lateral lymph node metastasis will be defined using preoperative MRI. The primary endpoint is 3-year disease-free survival (DFS). Secondary endpoints include 5-year DFS, local recurrence rate, systemic recurrence rate, cost-effectiveness, and overall survival. We hypothesized that our experimental group (arm B) will have a 3-year DFS of 75% and a non-inferiority margin of 15%.
Identifying whether patients require PCRT is one of the critical issues in locally advanced rectal cancer. This study aims to elucidate whether PCRT may not be required for all patients with stage II/III rectal cancer, especially for the MRI-based intermediate-risk group (with cTN or cTN) without CRM involvement and lateral lymph node metastasis. If the findings indicate that our proposed treatment, which omits PCRT, is non-inferior to the standard treatment, then patients may avoid unnecessary radiation-related toxicity, have a shorter treatment duration, and save on medical costs.
ClinicalTrials.gov, NCT02167321. Registered on 19 June 2014.
术前放化疗(PCRT)联合手术和辅助化疗是目前治疗 II/III 期直肠癌的标准治疗方法。然而,盆腔区域的放疗通常会导致吻合口漏、性功能障碍和粪便失禁等并发症。最近,MERCURY 研究表明,术前高分辨率磁共振成像(MRI)有助于选择性地避免 PCRT。目前尚不清楚对于单独手术即可获得阴性环周切缘(CRM)的患者以及 cTN 或 cTN 无 CRM 受累和侧方淋巴结转移的患者,是否需要进行 PCRT。本研究旨在评估术前根治性手术联合全直肠系膜切除术(TME)后辅助化疗(奥沙利铂、亚叶酸钙和氟尿嘧啶,FOLFOX)与目前标准治疗方法在可手术切除的局部进展期直肠癌患者中的疗效。
这项名为 TME-FOLFOX 的研究是一项前瞻性、开放标签、多中心、II 期随机试验。局部进展期直肠癌患者将被随机分配接受 PCRT 联合 TME 和辅助化疗(A 组)或术前根治性手术联合 TME 后辅助 FOLFOX 化疗(B 组)。无 CRM 受累和侧方淋巴结转移的临床 II/III 期直肠癌将通过术前 MRI 进行定义。主要终点是 3 年无病生存率(DFS)。次要终点包括 5 年 DFS、局部复发率、全身复发率、成本效益和总生存率。我们假设实验组(B 组)的 3 年 DFS 为 75%,非劣效性边界为 15%。
确定患者是否需要接受 PCRT 是局部进展期直肠癌的关键问题之一。本研究旨在阐明对于所有 II/III 期直肠癌患者,尤其是 MRI 显示的无 CRM 受累和侧方淋巴结转移的中间风险组(cTN 或 cTN)患者,是否不需要进行 PCRT。如果研究结果表明,我们提出的省略 PCRT 的治疗方案不劣于标准治疗方案,那么患者可以避免不必要的放射相关毒性,治疗时间更短,医疗费用更低。
ClinicalTrials.gov,NCT02167321。于 2014 年 6 月 19 日注册。