Department of Lifetime Clinical Immunology, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, 1-5-45 Yushima, Bunkyo-ku, Tokyo, 113-8519, Japan.
Department of Rheumatology, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, Tokyo, Japan.
Arthritis Res Ther. 2020 Apr 7;22(1):72. doi: 10.1186/s13075-020-02171-6.
Relapses frequently occur in giant cell arteritis (GCA), and long-term glucocorticoid therapy is required. The identification of associated factors with poor treatment outcomes is important to decide the treatment algorithm of GCA.
We enrolled 139 newly diagnosed GCA patients treated with glucocorticoids between 2007 and 2014 in a retrospective, multi-center registry. Patients were diagnosed with temporal artery biopsy, 1990 American College of Rheumatology classification criteria, or large vessel lesions (LVLs) detected by imaging based on the modified classification criteria. Poor treatment outcomes (non-achievement of clinical remission by week 24 or relapse during 52 weeks) were evaluated. Clinical remission was defined as the absence of clinical signs and symptoms in cranial and large vessel areas, polymyalgia rheumatica (PMR), and elevation of C-reactive protein (CRP) levels. A patient was determined to have a relapse if he/she had either one of the signs and symptoms that newly appeared or worsened after achieving clinical remission. Re-elevation of CRP without clinical manifestations was considered as a relapse if other causes such as infection were excluded and the treatment was intensified. Associated factors with poor treatment outcomes were analyzed by using the Cox proportional hazard model.
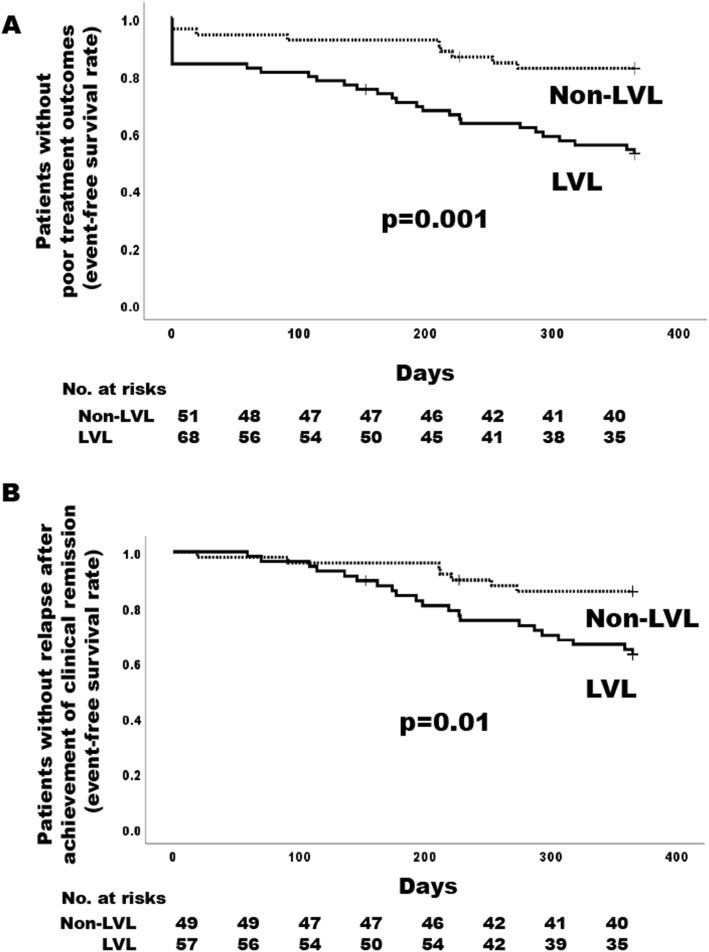
Cranial lesions, PMR, and LVLs were detected in 77.7%, 41.7%, and 52.5% of the enrolled patients, respectively. Treatment outcomes were evaluated in 119 newly diagnosed patients who were observed for 24 weeks or longer. The mean initial dose of prednisolone was 0.76 mg/kg/day, and 29.4% received any concomitant immunosuppressive drugs at baseline. Overall, 41 (34.5%) of the 119 patients had poor treatment outcomes; 13 did not achieve clinical remission by week 24, and 28 had a relapse after achieving clinical remission. Cumulative rates of the events of poor treatment outcomes in patients with and without LVLs were 47.5% and 17.7%, respectively. A multivariable model showed the presence of LVLs at baseline was significantly associated with poor treatment outcomes (adjusted hazard ratio [HR] 3.54, 95% CI 1.52-8.24, p = 0.003). Cranial lesions and PMR did not increase the risk of poor treatment outcomes.
The initial treatment intensity in the treatment algorithm of GCA could be determined based upon the presence or absence of LVLs detected by imaging at baseline.
巨细胞动脉炎(GCA)经常复发,需要长期使用糖皮质激素治疗。确定与不良治疗结果相关的因素对于决定 GCA 的治疗方案非常重要。
我们回顾性地纳入了 2007 年至 2014 年间在多中心登记处接受糖皮质激素治疗的 139 例新诊断的 GCA 患者。患者通过颞动脉活检、1990 年美国风湿病学会分类标准或基于改良分类标准的影像学检查发现的大血管病变(LVL)进行诊断。评估不良治疗结果(24 周未达到临床缓解或 52 周内复发)。临床缓解定义为颅部和大血管区域、巨细胞性多肌痛(PMR)无临床体征和症状以及 C 反应蛋白(CRP)水平升高。如果患者在达到临床缓解后出现新的或恶化的体征和症状,则认为发生了复发。如果排除感染等其他原因且强化治疗后 CRP 再次升高但无临床症状,则认为是复发。采用 Cox 比例风险模型分析与不良治疗结果相关的因素。
纳入的患者中分别有 77.7%、41.7%和 52.5%存在颅部病变、PMR 和 LVL。对 119 例新诊断的患者进行了 24 周或更长时间的观察,以评估治疗结果。泼尼松龙的初始剂量平均为 0.76mg/kg/天,29.4%的患者在基线时接受任何联合免疫抑制药物治疗。总体而言,119 例患者中有 41 例(34.5%)存在不良治疗结果;13 例在第 24 周未达到临床缓解,28 例在达到临床缓解后复发。有和没有 LVL 的患者不良治疗结果事件的累积发生率分别为 47.5%和 17.7%。多变量模型显示基线时存在 LVL 与不良治疗结果显著相关(调整后的危险比[HR]3.54,95%置信区间[CI]1.52-8.24,p=0.003)。颅部病变和 PMR 并未增加不良治疗结果的风险。
可以根据基线时影像学检查发现的 LVL 的存在与否来确定 GCA 治疗方案中的初始治疗强度。