Massachusetts General Hospital and Harvard Medical School, Boston, Massachusetts.
Genentech, San Francisco, California.
Arthritis Rheumatol. 2019 Aug;71(8):1329-1338. doi: 10.1002/art.40876. Epub 2019 Jul 3.
This study was undertaken to evaluate glucocorticoid dosages and serologic findings in patients with giant cell arteritis (GCA) flares.
Patients with GCA were randomly assigned to receive double-blind dosing with either subcutaneous tocilizumab (TCZ) 162 mg weekly plus 26-week prednisone taper (TCZ-QW + Pred-26), every-other-week TCZ plus 26-week prednisone taper (TCZ-Q2W + Pred-26), placebo plus 26-week prednisone taper (PBO + Pred-26), or placebo plus 52-week prednisone taper (PBO + Pred-52). Outcome measures were prednisone dosage, C-reactive protein (CRP) level, and erythrocyte sedimentation rate (ESR) at the time of flare.
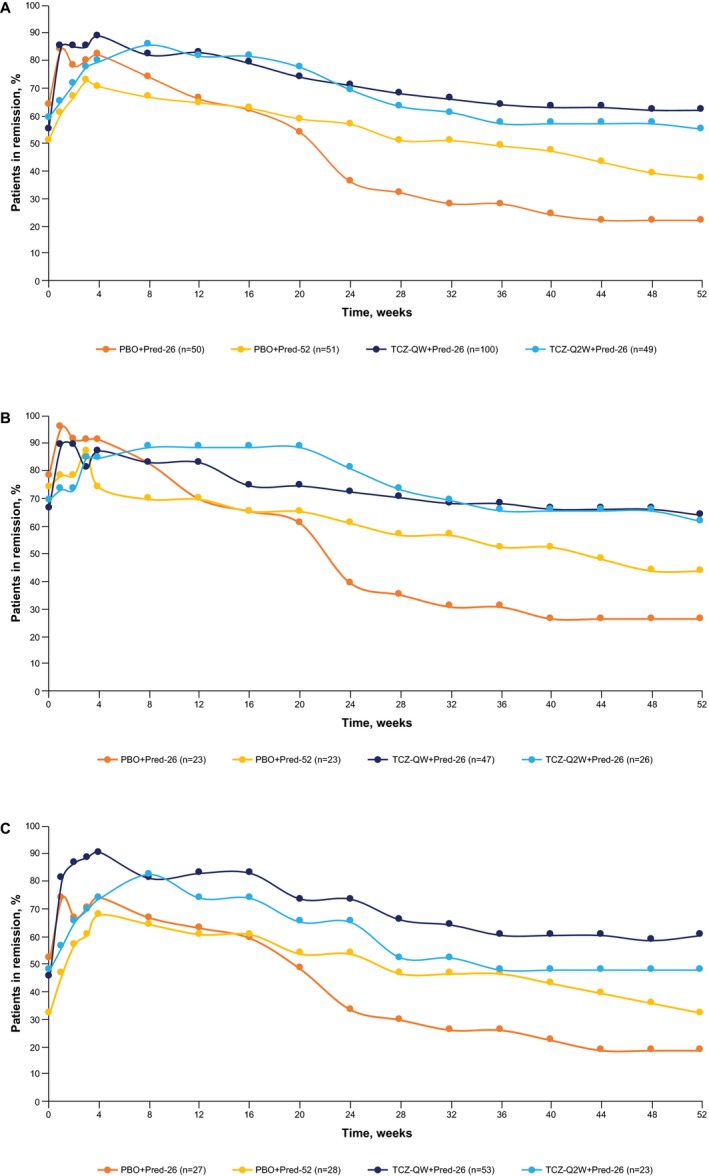
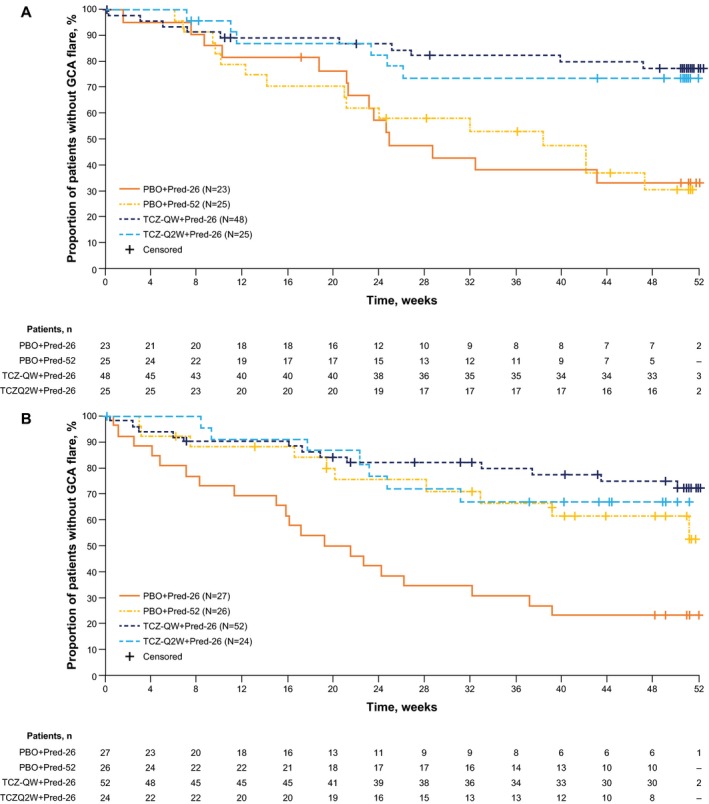
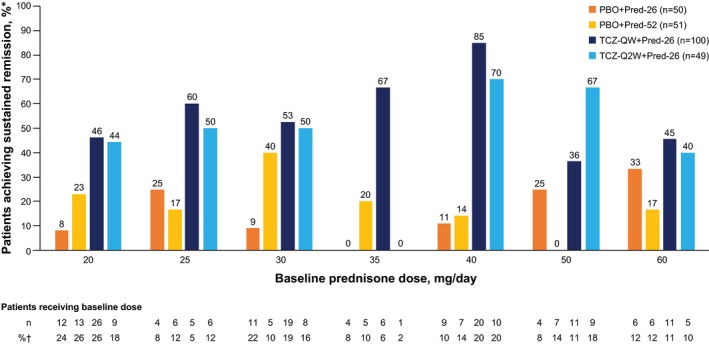
One hundred patients received TCZ-QW + Pred-26, 49 received TCZ-Q2W + Pred-26, 50 received PBO + Pred-26, and 51 received PBO + Pred-52. Of the 149 TCZ-treated patients, 36 (24%) experienced flare, 23 (64%) of whom were still receiving prednisone (median dosage 2.0 mg/day). Among 101 PBO + Pred-treated patients, 59 (58%) experienced flare, 45 (76%) of whom were receiving prednisone (median dosage 5.0 mg/day). Many flares occurred while patients were taking >10 mg/day prednisone: 9 (25%) in the TCZ groups and 13 (22%) in the placebo groups. Thirty-three flares (92%) in TCZ-treated groups and 20 (34%) in PBO + Pred-treated groups occurred with normal CRP levels. More than half of the PBO + Pred-treated patients had elevated CRP levels without flares. Benefits of the TCZ and prednisone combination over prednisone alone for remission induction were apparent by 8 weeks.
Most GCA flares occurred while patients were still receiving prednisone. Acute-phase reactant levels were not reliable indicators of flare in patients treated with TCZ plus prednisone or with prednisone alone. The addition of TCZ to prednisone facilitates earlier GCA control.
本研究旨在评估巨细胞动脉炎(GCA)发作患者的糖皮质激素剂量和血清学发现。
将 GCA 患者随机分配接受皮下托珠单抗(TCZ)162mg 每周一次加 26 周泼尼松减量(TCZ-QW+Pred-26)、每两周 TCZ 一次加 26 周泼尼松减量(TCZ-Q2W+Pred-26)、安慰剂加 26 周泼尼松减量(PBO+Pred-26)或安慰剂加 52 周泼尼松减量(PBO+Pred-52)的双盲剂量治疗。主要结局是发作时的泼尼松剂量、C 反应蛋白(CRP)水平和红细胞沉降率(ESR)。
100 例患者接受 TCZ-QW+Pred-26、49 例接受 TCZ-Q2W+Pred-26、50 例接受 PBO+Pred-26、51 例接受 PBO+Pred-52。在 149 例 TCZ 治疗患者中,36 例(24%)出现发作,其中 23 例(64%)仍在接受泼尼松治疗(中位剂量 2.0mg/天)。在 101 例 PBO+Pred 治疗患者中,59 例(58%)出现发作,其中 45 例(76%)接受泼尼松治疗(中位剂量 5.0mg/天)。许多发作发生在患者服用>10mg/天时:TCZ 组 9 例(25%),安慰剂组 13 例(22%)。在 TCZ 治疗组中,33 例(92%)和在 PBO+Pred 治疗组中 20 例(34%)的发作时 CRP 水平正常。超过一半的 PBO+Pred 治疗患者在没有发作时 CRP 水平升高。TCZ 和泼尼松联合治疗与单独使用泼尼松相比,在 8 周时对缓解诱导的益处更为明显。
大多数 GCA 发作发生在患者仍在接受泼尼松治疗时。急性反应物水平不能可靠地预测 TCZ 加泼尼松或单独使用泼尼松治疗患者的发作。在泼尼松中加入 TCZ 可更早地控制 GCA。