Clinicum, Faculty of Medicine, University of Helsinki, Helsinki, Finland.
Translational & Experimental Medicine, Early Respiratory, Inflammation and Autoimmunity, BioPharmaceuticals R&D, AstraZeneca, Gothenburg, Sweden.
Front Immunol. 2020 Mar 19;11:468. doi: 10.3389/fimmu.2020.00468. eCollection 2020.
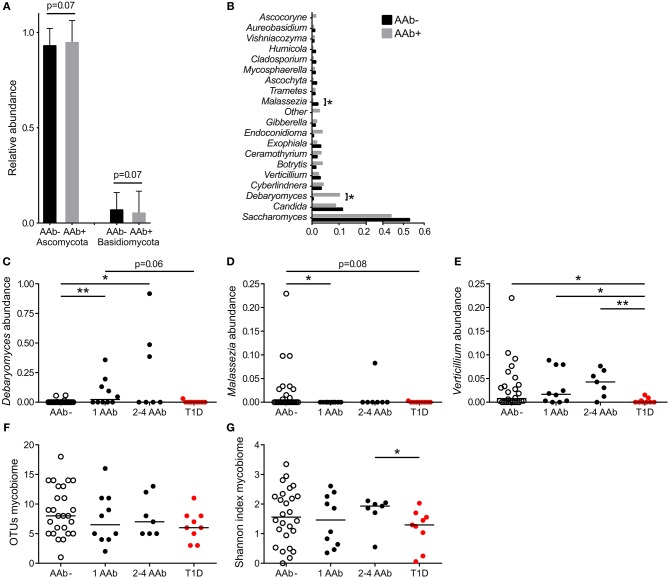
Although gut bacterial dysbiosis is recognized as a regulator of beta-cell autoimmunity, no data is available on fungal dysbiosis in the children at the risk of type 1 diabetes (T1D). We hypothesized that the co-occurrence of fungal and bacterial dysbiosis contributes to the intestinal inflammation and autoimmune destruction of insulin-producing beta-cells in T1D. Fecal and blood samples were collected from 26 children tested positive for at least one diabetes-associated autoantibody (IAA, GADA, IA-2A or ICA) and matched autoantibody-negative children with HLA-conferred susceptibility to T1D (matched for HLA-DQB1 haplotype, age, gender and early childhood nutrition). Bacterial 16S and fungal ITS2 sequencing, and analyses of the markers of intestinal inflammation, namely fecal human beta-defensin-2 (HBD2), calprotectin and secretory total IgA, were performed. Anti-Saccharomyces cerevisiae antibodies (ASCA) and circulating cytokines, IFNG, IL-17 and IL-22, were studied. After these analyses, the children were followed for development of clinical T1D (median 8 years and 8 months). Nine autoantibody positive children were diagnosed with T1D, whereas none of the autoantibody negative children developed T1D during the follow-up. Fungal dysbiosis, characterized by high abundance of fecal and , was found in the progressors, i.e., children with beta-cell autoimmunity who during the follow-up progressed to clinical T1D. These children showed also bacterial dysbiosis, i.e., increased Bacteroidales and Clostridiales ratio, which was, however, found also in the non-progressors, and is thus a common nominator in the children with beta-cell autoimmunity. Furthermore, the progressors showed markers of intestinal inflammation detected as increased levels of fecal HBD2 and ASCA IgG to fungal antigens. We conclude that the fungal and bacterial dysbiosis, and intestinal inflammation are associated with the development of T1D in children with beta-cell autoimmunity.
虽然肠道细菌失调被认为是调节β细胞自身免疫的因素,但目前尚无 1 型糖尿病(T1D)患儿中真菌失调的数据。我们假设真菌和细菌失调的共同发生导致 T1D 中肠道炎症和产生胰岛素的β细胞的自身免疫破坏。从 26 名至少有一种糖尿病相关自身抗体(IAA、GADA、IA-2A 或 ICA)阳性的儿童和与 HLA 赋予 T1D 易感性相匹配的自身抗体阴性儿童(匹配 HLA-DQB1 单倍型、年龄、性别和儿童早期营养)中采集粪便和血液样本。进行了细菌 16S 和真菌 ITS2 测序,以及肠道炎症标志物的分析,即粪便人β防御素-2(HBD2)、钙卫蛋白和分泌总 IgA。研究了抗酿酒酵母抗体(ASCA)和循环细胞因子 IFNG、IL-17 和 IL-22。在这些分析之后,对儿童进行了 T1D 的临床发展(中位数为 8 年 8 个月)。9 名自身抗体阳性儿童被诊断为 T1D,而在随访期间,无自身抗体阴性儿童发展为 T1D。在进展者中发现了真菌失调,其特征是粪便中 和 的丰度高,即具有β细胞自身免疫的儿童在随访期间进展为临床 T1D。这些儿童还表现出细菌失调,即增加的拟杆菌门和梭状芽孢杆菌门的比例,但这也在非进展者中发现,因此是β细胞自身免疫儿童的常见共同因素。此外,进展者表现出肠道炎症标志物的增加,如粪便 HBD2 和抗真菌抗原的 ASCA IgG 水平升高。我们得出结论,真菌和细菌失调以及肠道炎症与具有β细胞自身免疫的儿童 T1D 的发展有关。