Department of Neurological Surgery, Mayo Clinic, Rochester, Minnesota.
Division of Endocrinology, Indiana University, Indianapolis, Indiana.
Neurosurgery. 2020 Sep 1;87(3):538-546. doi: 10.1093/neuros/nyaa054.
Stereotactic radiosurgery (SRS) is a safe and effective treatment for acromegaly.
To improve understanding of clinical and dosimetric factors predicting biochemical remission.
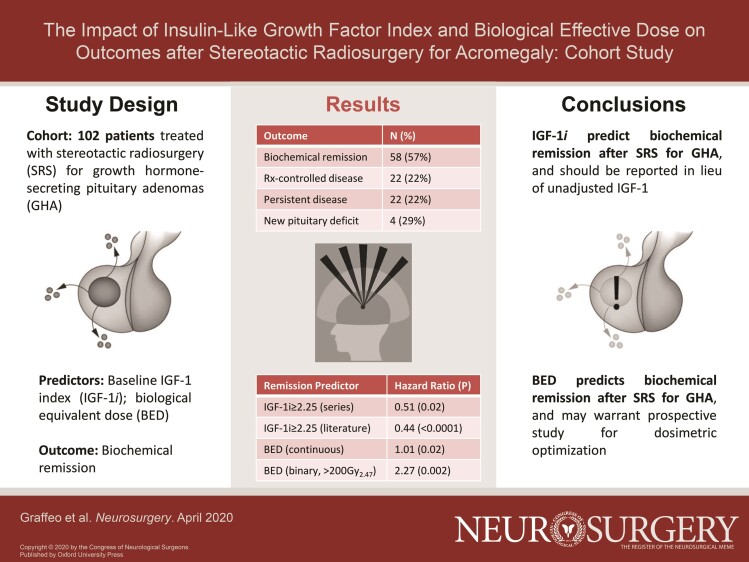
A single-institution cohort study of nonsyndromic, radiation-naïve patients with growth hormone-producing pituitary adenomas (GHA) having single-fraction SRS between 1990 and 2017. Exclusions were treatment with pituitary suppressive medications at the time of SRS, or <24 mo of follow-up. The primary outcome was biochemical remission-defined as normalization of insulin-like growth factor-1 index (IGF-1i) off suppression. Biochemical remission was assessed using Cox proportional hazards. Prior studies reporting IGF-1i were assessed via systematic literature review and meta-analysis using random-effect modeling.
A total of 102 patients met study criteria. Of these, 46 patients (45%) were female. The median age was 49 yr (interquartile range [IQR] = 37-59), and the median follow-up was 63 mo (IQR = 29-100). The median pre-SRS IGF-1i was 1.66 (IQR = 1.37-3.22). The median margin dose was 25 Gy (IQR = 21-25); the median estimated biologically effective dose (BED) was 169.49 Gy (IQR = 124.95-196.00). Biochemical remission was achieved in 58 patients (57%), whereas 22 patients (22%) had medication-controlled disease. Pre-SRS IGF-1i ≥ 2.25 was the strongest predictor of treatment failure, with an unadjusted hazard ratio (HR) of 0.51 (95% CI = 0.26-0.91, P = .02). Number of isocenters, margin dose, and BED predicted remission on univariate analysis, but after adjusting for sex and baseline IGF-1i, only BED remained significant-and was independently associated with outcome in continuous (HR = 1.01, 95% CI = 1.00-1.01, P = .02) and binary models (HR = 2.27, 95% CI = 1.39-5.22, P = .002). A total of 24 patients (29%) developed new post-SRS hypopituitarism. Pooled HR for biochemical remission given subthreshold IGF-1i was 2.25 (95% CI = 1.33-3.16, P < .0001).
IGF-1i is a reliable predictor of biochemical remission after SRS. BED appears to predict biochemical outcome more reliably than radiation dose, but confirmatory study is needed.
立体定向放射外科(SRS)是治疗肢端肥大症的一种安全有效的治疗方法。
提高对预测生化缓解的临床和剂量学因素的理解。
对 1990 年至 2017 年间接受单次分割 SRS 的非综合征性、放射治疗初治生长激素分泌垂体腺瘤(GHA)的单机构队列研究。排除标准为 SRS 时使用垂体抑制药物治疗或随访时间<24 个月。主要结局是生化缓解定义为胰岛素样生长因子 1 指数(IGF-1i)抑制后正常化。采用 Cox 比例风险评估生化缓解。通过系统文献回顾和使用随机效应模型的荟萃分析评估先前报告 IGF-1i 的研究。
共有 102 例患者符合研究标准。其中,46 例(45%)为女性。中位年龄为 49 岁(四分位距[IQR] = 37-59),中位随访时间为 63 个月(IQR = 29-100)。SRS 前 IGF-1i 的中位数为 1.66(IQR = 1.37-3.22)。中位边缘剂量为 25 Gy(IQR = 21-25);中位估计生物有效剂量(BED)为 169.49 Gy(IQR = 124.95-196.00)。58 例患者(57%)达到生化缓解,22 例患者(22%)疾病得到药物控制。SRS 前 IGF-1i≥2.25 是治疗失败的最强预测因素,未调整的风险比(HR)为 0.51(95%CI = 0.26-0.91,P = 0.02)。在单变量分析中,照射的等中心点数量、边缘剂量和 BED 预测缓解,但在调整性别和基线 IGF-1i 后,仅 BED 仍具有统计学意义-并且与连续(HR = 1.01,95%CI = 1.00-1.01,P = 0.02)和二进制模型(HR = 2.27,95%CI = 1.39-5.22,P = 0.002)的结果独立相关。共有 24 例患者(29%)在 SRS 后出现新的垂体功能减退症。IGF-1i 亚阈值时生化缓解的汇总 HR 为 2.25(95%CI = 1.33-3.16,P<0.0001)。
IGF-1i 是 SRS 后生化缓解的可靠预测因子。BED 似乎比剂量更可靠地预测生化结果,但需要进一步的确认性研究。