Division of Cancer Epidemiology and Genetics, Clinical Genetics Branch, National Cancer Institute, Rockville, MD.
Department of Obstetrics and Gynecology, George Washington School of Medicine, Washington, DC.
Am J Obstet Gynecol. 2020 Oct;223(4):549.e1-549.e13. doi: 10.1016/j.ajog.2020.03.032. Epub 2020 Apr 5.
Most endometrial cancer cases are preceded by abnormal uterine bleeding, offering a potential opportunity for early detection and cure of endometrial cancer. Although clinical guidelines exist for diagnostic workup of abnormal uterine bleeding, consensus is lacking regarding optimal management for women with abnormal bleeding to diagnose endometrial cancer.
We report the baseline data from a prospective clinical cohort study of women referred for endometrial evaluation at the Mayo Clinic, designed to evaluate risk stratification in women at increased risk for endometrial cancer. Here, we introduce a risk-based approach to evaluate diagnostic tests and clinical management algorithms in a population of women with abnormal bleeding undergoing endometrial evaluation at the Mayo Clinic.
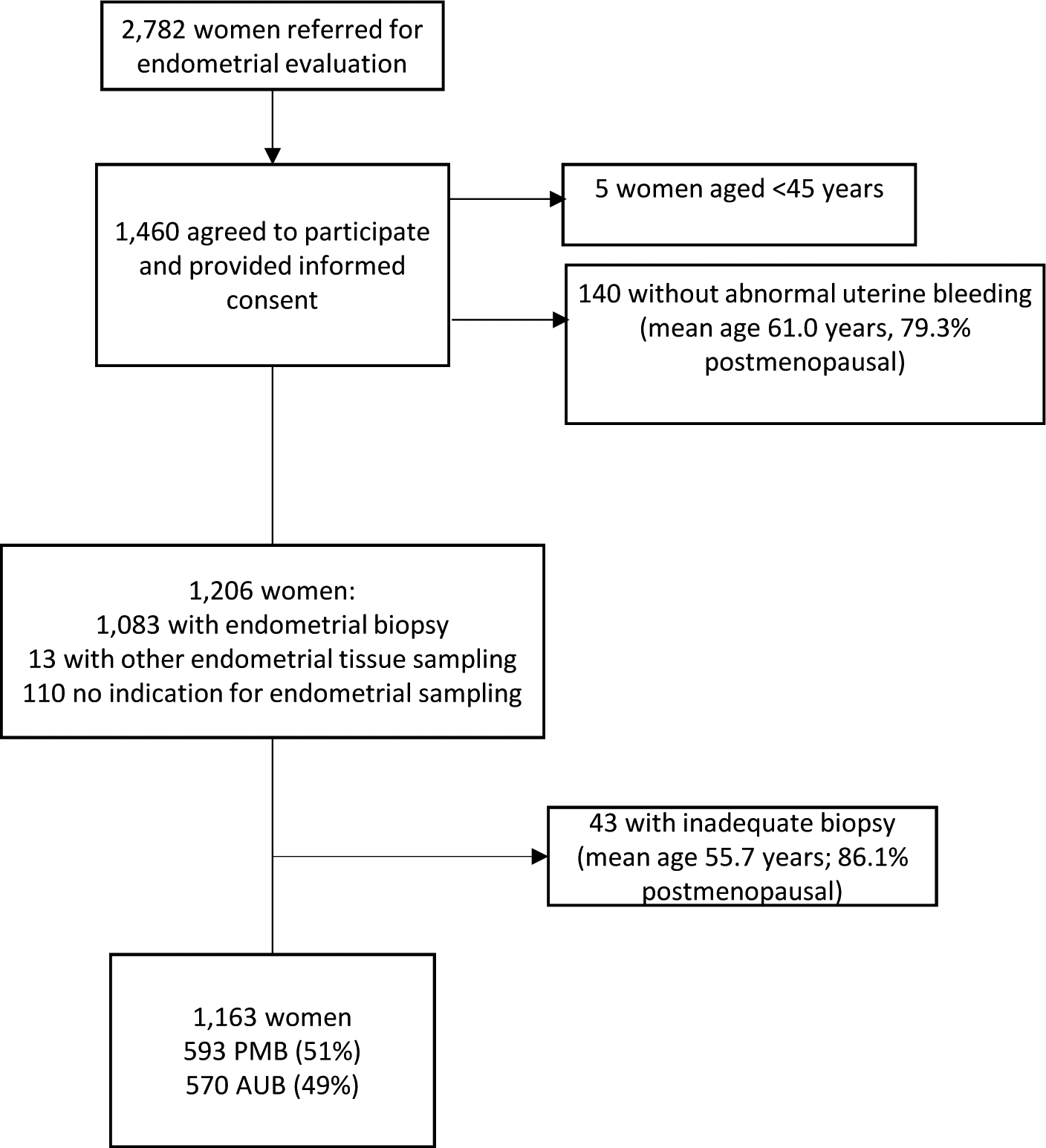
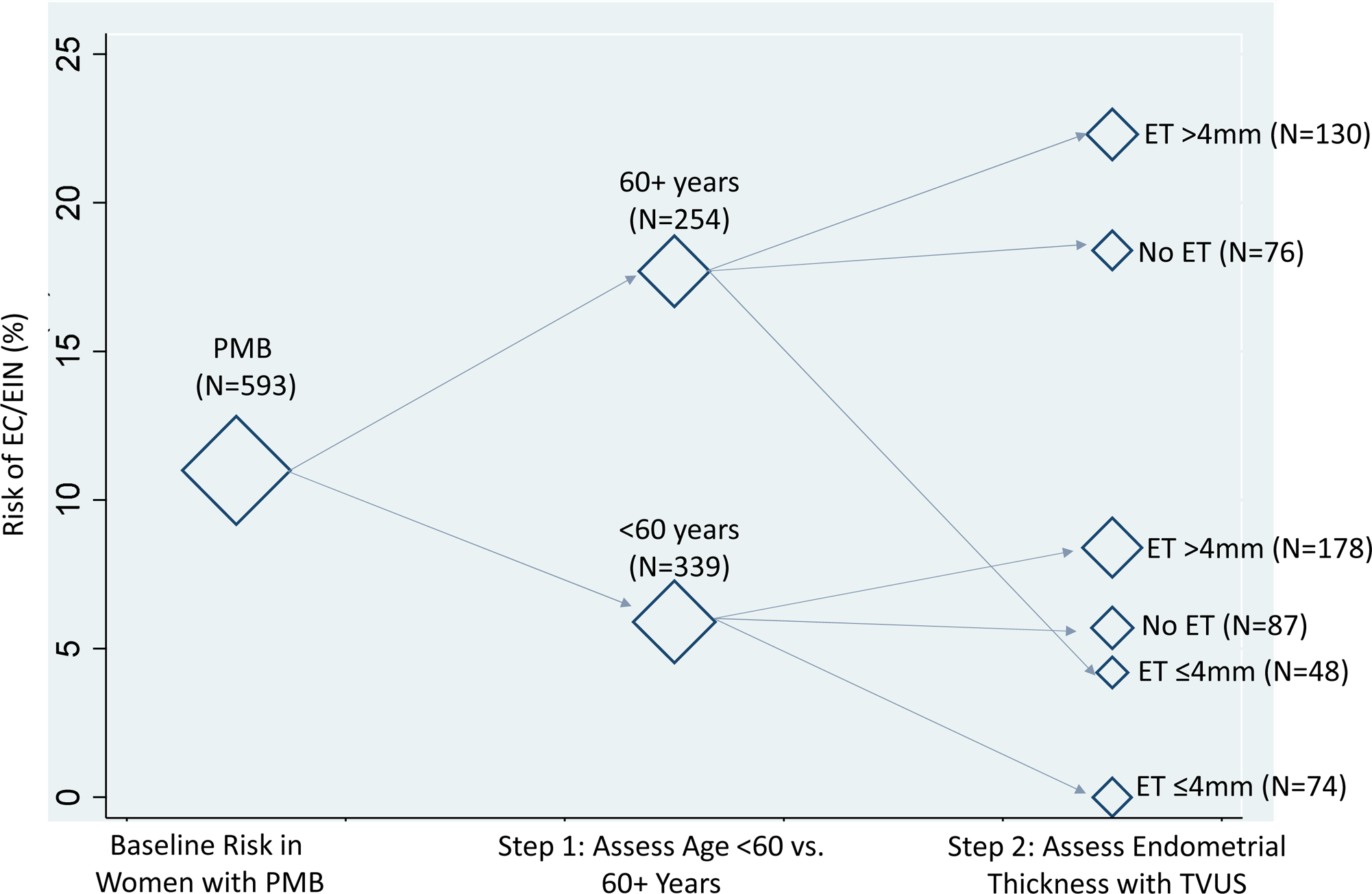
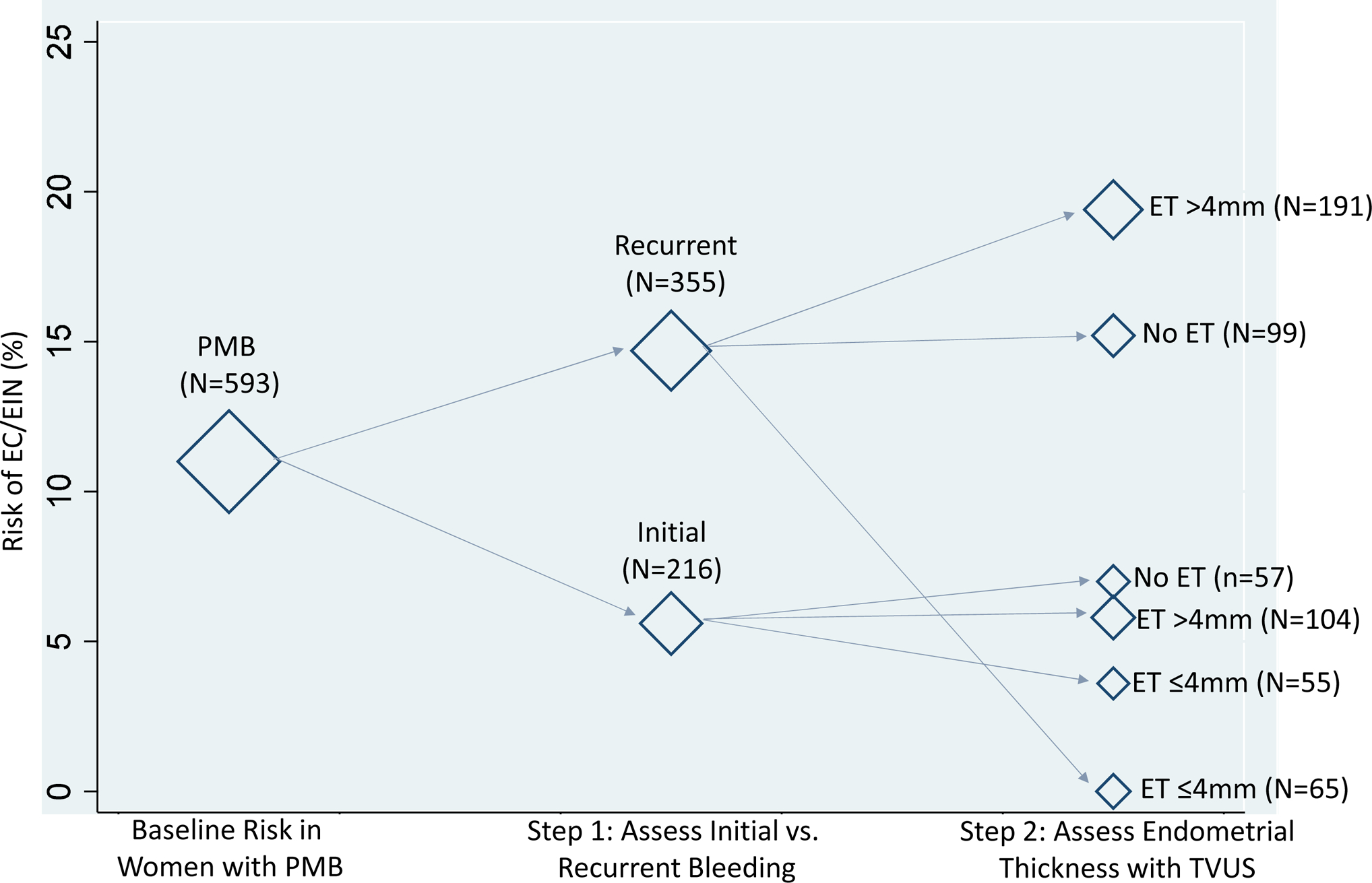
A total of 1163 women aged ≥45 years were enrolled from February 2013 to May 2019. We evaluated baseline absolute risks and 95% confidence intervals of endometrial cancer and endometrial intraepithelial neoplasia according to clinical algorithms for diagnostic workup of women with postmenopausal bleeding (assessment of initial vs recurrent bleeding episode and endometrial thickness measured through transvaginal ultrasound). We also evaluated risks among women with postmenopausal bleeding according to baseline age (<60 vs 60+ years) as an alternative example. For this approach, biopsy would be conducted for all women aged 60+ years and those aged <60 years with an endometrial thickness of >4 mm. We assessed the clinical efficiency of each strategy by estimating the percentage of women who would be referred for endometrial biopsy, the percentage of cases detected and missed, and the ratio of biopsies per case detected.
Among the 593 women with postmenopausal bleeding, 18 (3.0%) had endometrial intraepithelial neoplasia, and 47 (7.9%) had endometrial cancer, and among the 570 premenopausal women with abnormal bleeding, 8 (1.4%) had endometrial intraepithelial neoplasia, and 7 (1.2%) had endometrial cancer. Maximum risk was noted in women aged 60+ years (17.7%; 13.0%-22.3%), followed by those with recurrent bleeding (14.7%; 11.0%-18.3%). Among women with an initial bleeding episode for whom transvaginal ultrasound was recommended, endometrial thickness did not provide meaningful risk stratification: risks of endometrial cancer and endometrial intraepithelial neoplasia were nearly identical in women with an endometrial thickness of >4 mm (5.8%; 1.3%-10.3%) and ≤4 mm (3.6%; 0.9%-8.6%). In contrast, among those aged <60 years with an endometrial thickness of >4 mm, the risk of endometrial cancer and endometrial intraepithelial neoplasia was 8.4% (4.3%-12.5%), and in those with an endometrial thickness of ≤4 mm, the risk was 0% (0.0%-3.0%; P=.01). The most efficient strategy was to perform biopsy in all women aged 60+ years and among those aged <60 years with an endometrial thickness of >4 mm, with the lowest percentage referred to biopsy while still detecting all cases.
Existing clinical recommendations for endometrial cancer detection in women with abnormal bleeding are not consistent with the underlying risk. Endometrial cancer risk factors such as age can provide important risk stratification compared with the assessment of recurrent bleeding. Future research will include a formal assessment of clinical and epidemiologic risk prediction models in our study population as well as validation of our findings in other populations.
大多数子宫内膜癌病例之前都有异常子宫出血,这为子宫内膜癌的早期发现和治疗提供了潜在机会。虽然有针对异常子宫出血的诊断性检查的临床指南,但对于有异常出血症状的女性,如何最佳管理以诊断子宫内膜癌,目前仍缺乏共识。
我们报告了梅奥诊所前瞻性临床队列研究中女性子宫内膜评估的基线数据,该研究旨在评估子宫内膜癌风险分层。在这里,我们引入了一种基于风险的方法,以评估在梅奥诊所接受子宫内膜评估的异常出血女性中诊断性检查和临床管理算法。
共有 1163 名年龄≥45 岁的女性于 2013 年 2 月至 2019 年 5 月入组。我们根据绝经后出血的诊断性检查临床算法(评估初始与复发出血事件和经阴道超声测量的子宫内膜厚度)评估了绝经后出血女性的子宫内膜癌和子宫内膜上皮内瘤变的绝对风险和 95%置信区间。我们还根据基线年龄(<60 岁与≥60 岁)评估了绝经后出血女性的风险。对于这种方法,所有年龄≥60 岁的女性和年龄<60 岁且子宫内膜厚度>4 mm 的女性都将进行活检。我们通过估计将进行子宫内膜活检的女性百分比、检测到的病例和漏诊的病例百分比以及每例检测到的病例进行活检的比例来评估每种策略的临床效率。
在 593 名绝经后出血的女性中,有 18 名(3.0%)患有子宫内膜上皮内瘤变,47 名(7.9%)患有子宫内膜癌;在 570 名异常出血的绝经前女性中,有 8 名(1.4%)患有子宫内膜上皮内瘤变,7 名(1.2%)患有子宫内膜癌。最大风险发生在年龄≥60 岁的女性(17.7%;13.0%-22.3%),其次是复发出血的女性(14.7%;11.0%-18.3%)。对于建议进行经阴道超声检查的有初始出血症状的女性,子宫内膜厚度不能提供有意义的风险分层:在子宫内膜厚度>4 mm(5.8%;1.3%-10.3%)和≤4 mm(3.6%;0.9%-8.6%)的女性中,子宫内膜癌和子宫内膜上皮内瘤变的风险几乎相同。相比之下,在年龄<60 岁且子宫内膜厚度>4 mm 的女性中,子宫内膜癌和子宫内膜上皮内瘤变的风险为 8.4%(4.3%-12.5%),而在子宫内膜厚度≤4 mm 的女性中,风险为 0%(0.0%-3.0%;P=.01)。最有效的策略是对所有年龄≥60 岁的女性和年龄<60 岁且子宫内膜厚度>4 mm 的女性进行活检,该策略转诊进行活检的比例最低,同时仍能检测到所有病例。
目前针对异常出血女性进行子宫内膜癌检测的临床建议与潜在风险不一致。与评估复发出血相比,年龄等子宫内膜癌危险因素可以提供重要的风险分层。未来的研究将包括在我们的研究人群中对临床和流行病学风险预测模型进行正式评估,以及在其他人群中验证我们的发现。