Cohen Stanley, Tuckwell Katie, Katsumoto Tamiko R, Zhao Rui, Galanter Joshua, Lee Chin, Rae Julie, Toth Balazs, Ramamoorthi Nandhini, Hackney Jason A, Berman Alberto, Damjanov Nemanja, Fedkov Dmytro, Jeka Slawomir, Chinn Leslie W, Townsend Michael J, Morimoto Alyssa M, Genovese Mark C
Metroplex Clinical Research Center, Dallas, TX, USA.
Genentech, Inc, South San Francisco, CA, USA.
Arthritis Rheumatol. 2020 Apr 9;72(9):1435-46. doi: 10.1002/art.41275.
To evaluate fenebrutinib, an oral and highly selective non-covalent inhibitor of Bruton's tyrosine kinase (BTK), in patients with active rheumatoid arthritis (RA).
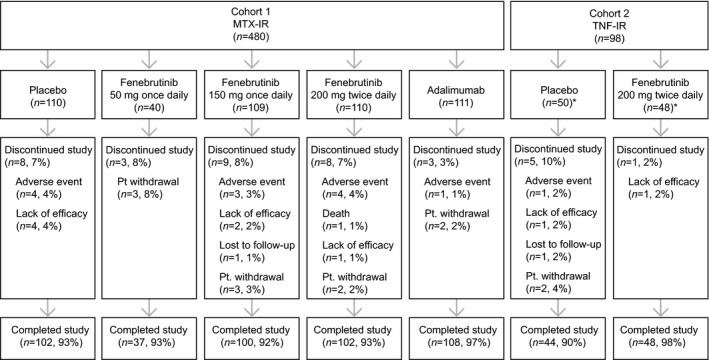
Patients with RA and inadequate response to methotrexate (cohort 1, n=480) were randomized to fenebrutinib (50 mg once daily, 150 mg once daily, 200 mg twice daily), 40 mg adalimumab every other week, or placebo. Patients with RA and inadequate response to tumor necrosis factor inhibitors (cohort 2, n=98) received fenebrutinib (200 mg twice daily) or placebo. Both cohorts continued methotrexate therapy.
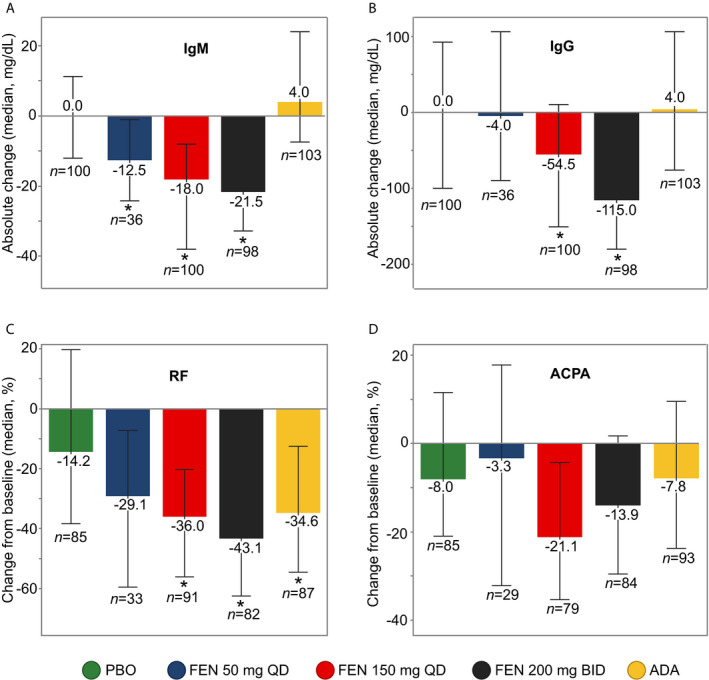
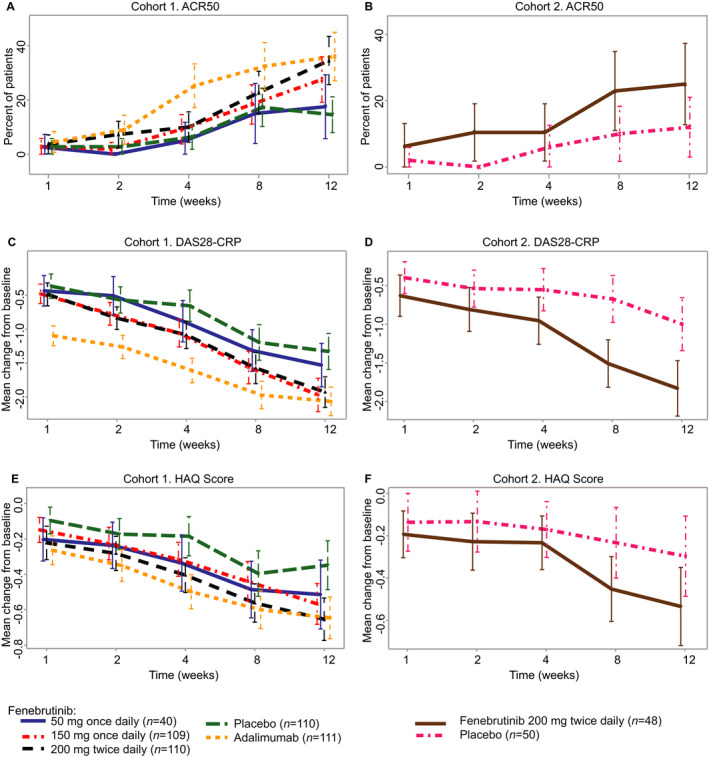
In cohort 1, American College of Rheumatology scores (ACR50) at week 12 were similar for fenebrutinib 50 mg once daily and placebo, and higher for fenebrutinib 150 mg once daily (28%) and 200 mg twice daily (35%) than placebo (15%) (p=0.017; p=0.0003). Fenebrutinib 200 mg twice daily and adalimumab (36%) were comparable (p=0.81). In cohort 2, more patients achieved ACR50 with fenebrutinib 200 mg twice daily (25%) than placebo (12%) (p=0.072). The most common adverse events for fenebrutinib included nausea, headache, anemia, and upper respiratory tract infections. Fenebrutinib had significant effects on myeloid and B cell biomarkers (CCL4 and rheumatoid factor). Fenebrutinib and adalimumab caused overlapping as well as distinct changes in B cell and myeloid biomarkers.
Fenebrutinib demonstrated efficacy comparable to adalimumab in patients with an inadequate response to methotrexate, and safety consistent with existing immunomodulatory therapies for RA. These data support targeting both B and myeloid cells via this novel mechanism for potential efficacy in the treatment of RA.
评估口服且高度选择性的布鲁顿酪氨酸激酶(BTK)非共价抑制剂非奈布替尼在活动性类风湿关节炎(RA)患者中的疗效。
对甲氨蝶呤治疗反应不足的RA患者(队列1,n = 480)被随机分为非奈布替尼组(每日一次50毫克、每日一次150毫克、每日两次200毫克)、每两周一次40毫克阿达木单抗组或安慰剂组。对肿瘤坏死因子抑制剂治疗反应不足的RA患者(队列2,n = 98)接受非奈布替尼(每日两次200毫克)或安慰剂治疗。两个队列均继续甲氨蝶呤治疗。
在队列1中,第12周时,每日一次50毫克非奈布替尼组的美国风湿病学会评分(ACR50)与安慰剂组相似,每日一次150毫克非奈布替尼组(28%)和每日两次200毫克非奈布替尼组(35%)高于安慰剂组(15%)(p = 0.017;p = 0.0003)。每日两次200毫克非奈布替尼组与阿达木单抗组(36%)相当(p = 0.81)。在队列2中,每日两次200毫克非奈布替尼组达到ACR50的患者(25%)多于安慰剂组(12%)(p = 0.072)。非奈布替尼最常见的不良事件包括恶心、头痛、贫血和上呼吸道感染。非奈布替尼对髓系和B细胞生物标志物(CCL4和类风湿因子)有显著影响。非奈布替尼和阿达木单抗在B细胞和髓系生物标志物上引起了重叠以及不同的变化。
在对甲氨蝶呤治疗反应不足的患者中,非奈布替尼显示出与阿达木单抗相当的疗效,且安全性与现有的RA免疫调节疗法一致。这些数据支持通过这种新机制同时靶向B细胞和髓系细胞,在RA治疗中具有潜在疗效。