Gala-Błądzińska Agnieszka, Romanek Janusz, Mazur Danuta, Stepek Tomasz, Braun Marcin, Szafarz Piotr, Chlebuś Marcin, Przybylski Andrzej
Medical College of Rzeszów University, Institute of Medical Sciences, Rzeszów 35-310, Poland.
Department of Internal Medicine, Nephrology and Endocrinology, St. Queen Jadwiga Clinical District Hospital No. 2 in Rzeszów, Rzeszów 35-301, Poland.
Cardiol Res Pract. 2020 Mar 21;2020:2727108. doi: 10.1155/2020/2727108. eCollection 2020.
Patients with chronic cardiorenal syndrome type 2 (T2-CRS) who qualify for resynchronization therapy (CRT) are exposed perioperatively to potentially nephrotoxic factors including contrast agents and blood loss.
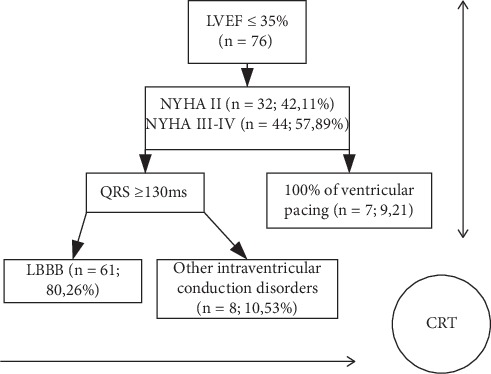
The objective of this prospective interventional study was to assess the effects of CRT on renal function in patients with T2-CRS within the first 48 hours following implantation. Initially, 76 patients (15% female; aged 69 ± 9.56 years) with heart failure (New York Heart Association classes II-IV), ejection fraction ≤ 35%, and QRS > 130 ms were included in the study. During CRT implantation, a nonionic contrast agent (72.2 ± 44.9 mL) was administered. Prior to and 48 hours following implantation, renal function was evaluated using the following serum biomarkers: creatinine (sCr), estimated glomerular filtration rate (using the Chronic Kidney Disease Epidemiology Collaboration equation [eGFR]), and the electrolyte and urine biomarkers albumin (uAlb), albumin/creatinine ratio (UACR), and neutrophil gelatinase-associated lipocalin (uNGAL).
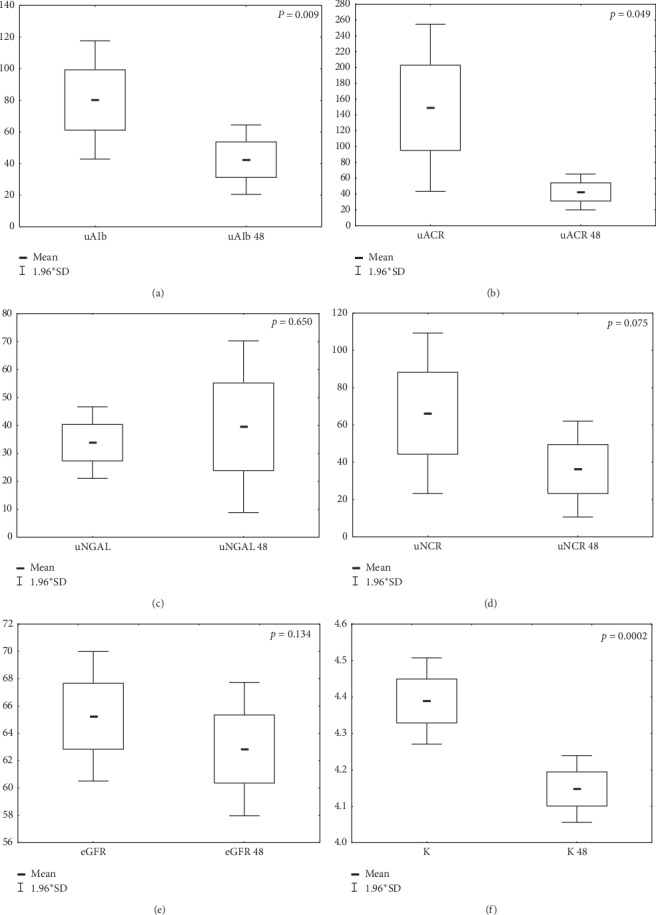
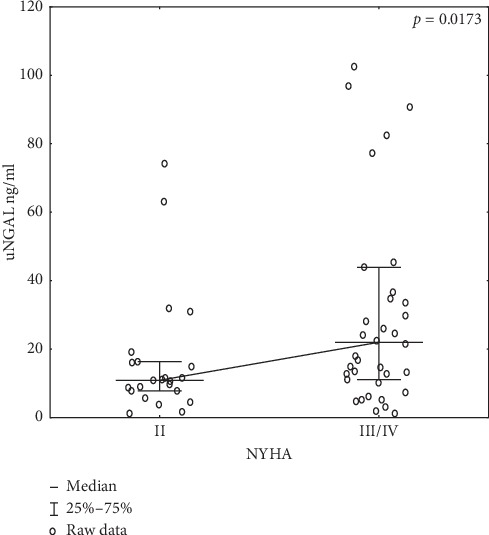
Before CRT, patients classified as NYHA class III or IV had higher uNGAL levels in comparison to uNGAL levels after CRT (43.63 ± 60.02 versus 16.63 ± 18.19; =0.041). After CRT implantation, uAlb, UACR, and potassium levels were reduced ( < 0.05), and uNGAL, sCr, and eGFR were unchanged. The contrast medium volume did not correlate with the test biomarkers ( > 0.05).
In patients with T2-CRS, uNGAL is a biomarker of kidney injury that correlates with the NYHA classes. A stable uNGAL value before and after CRT implantation confirms the lack of risk of contrast-induced nephropathy. Reduced albuminuria and blood potassium are biomarkers of improving T2-CRS in the early post-CRT period.
符合心脏再同步治疗(CRT)条件的慢性心肾综合征2型(T2-CRS)患者在围手术期会接触到潜在的肾毒性因素,包括造影剂和失血。
这项前瞻性干预研究的目的是评估CRT对T2-CRS患者植入后最初48小时内肾功能的影响。最初,76例患者(15%为女性;年龄69±9.56岁)纳入研究,这些患者患有心力衰竭(纽约心脏协会II-IV级)、射血分数≤35%且QRS>130毫秒。在CRT植入过程中,给予非离子型造影剂(72.2±44.9毫升)。在植入前和植入后48小时,使用以下血清生物标志物评估肾功能:肌酐(sCr)、估计肾小球滤过率(使用慢性肾脏病流行病学协作方程[eGFR])以及电解质和尿液生物标志物白蛋白(uAlb)、白蛋白/肌酐比值(UACR)和中性粒细胞明胶酶相关脂质运载蛋白(uNGAL)。
在CRT之前,与CRT之后相比,纽约心脏协会III级或IV级患者的uNGAL水平更高(43.63±60.02对16.63±18.19;P=0.041)。CRT植入后,uAlb、UACR和钾水平降低(P<0.05),而uNGAL、sCr和eGFR未改变。造影剂体积与检测生物标志物无相关性(P>0.05)。
在T2-CRS患者中,uNGAL是与纽约心脏协会分级相关的肾损伤生物标志物。CRT植入前后uNGAL值稳定证实不存在造影剂诱导的肾病风险。蛋白尿和血钾降低是CRT后早期T2-CRS改善的生物标志物。