Zwiers Alexandra J M, de Wildt Saskia N, van Rosmalen Joost, de Rijke Yolanda B, Buijs Erik A B, Tibboel Dick, Cransberg Karlien
Intensive Care and Department of Pediatric Surgery, Wytemaweg 80, 3015 CN, Rotterdam, the Netherlands.
Department of Pediatric Nephrology, Erasmus Medical Center-Sophia Children's Hospital, Wytemaweg 80, 3015 CN, Rotterdam, the Netherlands.
Crit Care. 2015 Apr 21;19(1):181. doi: 10.1186/s13054-015-0910-0.
Children admitted to a pediatric intensive care unit (ICU) are at high risk of developing acute kidney injury (AKI). Although serum creatinine (SCr) levels are used in clinical practice, they are insensitive for early diagnosis of AKI. Urinary neutrophil gelatinase-associated lipocalin (uNGAL) and kidney injury molecule-1 (KIM-1) are novel AKI biomarkers whose performance in pediatric ICU patients is largely unknown. In this study, we aimed to characterize uNGAL and KIM-1 patterns in children following ICU admission and to assess their properties in relation to identifying children at risk for AKI development.
From June 2010 until January 2014, we conducted a prospective observational cohort study of term-born children ages 1 day to 1 year on mechanical ventilation. Blood and urine samples were obtained every 6 to 12 hours up to 72 hours post-admission. Blood samples were assayed for SCr, and urine samples were assayed for uNGAL and KIM-1. The RIFLE (risk, injury, failure, loss, end-stage renal disease) classification as 150%, 200% or 300% of median SCr reference values was used to define AKI.
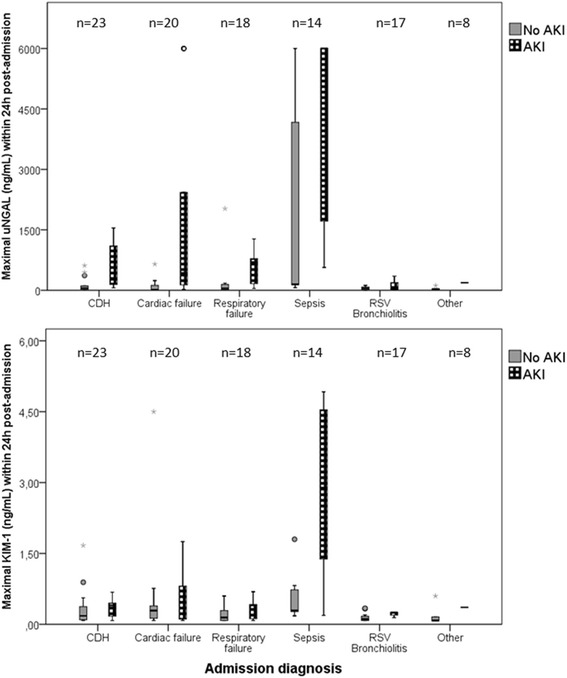
A total of 100 children were included (80 survived). Their median age at admission was 27.7 days (interquartile range (IQR), 1.5 to 85.5). The median duration of mechanical ventilation was 5.8 days (IQR, 3.1 to 11.4). Thirty-five patients had evidence of AKI within the first 48 hours post-admission, of whom 24 (69%) already had AKI when they entered the ICU. uNGAL and KIM-1 concentrations in AKI peaked between 6 to 12 hours and between 12 to 24 hours post-admission, respectively. The maximal area under the receiver operating characteristic curve (AUC) for uNGAL was 0.815 (95% confidence interval (CI), 0.685 to 0.945, P < 0.001) at 0 to 6 hours post-admission. The discriminative ability of KIM-1 was moderate, with a largest AUC of 0.737 (95% CI, 0.628 to 0.847; P < 0.001) at 12 to 24 hours post-admission. At the optimal cutoff point (126 ng/ml), uNGAL concentration predicted AKI development correctly in 16 (84%) of 19 children, up to 24 hours before a rise in SCr became apparent.
Levels of uNGAL and KIM-1 increase in patients with AKI following ICU admission and peak at 6 to 12 hours and 12 to 24 hours post-admission, respectively. uNGAL seems to be a reliable marker for identifying children who will develop AKI 24 hours later.
入住儿科重症监护病房(ICU)的儿童发生急性肾损伤(AKI)的风险很高。虽然血清肌酐(SCr)水平在临床实践中被使用,但它们对AKI的早期诊断并不敏感。尿中性粒细胞明胶酶相关脂质运载蛋白(uNGAL)和肾损伤分子-1(KIM-1)是新型的AKI生物标志物,其在儿科ICU患者中的表现很大程度上尚不清楚。在本研究中,我们旨在描述入住ICU后儿童的uNGAL和KIM-1模式,并评估它们在识别有发生AKI风险儿童方面的特性。
从2010年6月至2014年1月,我们对1日龄至1岁接受机械通气的足月儿进行了一项前瞻性观察队列研究。入院后72小时内每6至12小时采集一次血液和尿液样本。检测血液样本中的SCr,检测尿液样本中的uNGAL和KIM-1。采用将SCr参考值中位数的150%、200%或300%作为标准的RIFLE(风险、损伤、衰竭、丧失、终末期肾病)分类来定义AKI。
共纳入100名儿童(80名存活)。他们入院时的中位年龄为27.7天(四分位间距(IQR),1.5至85.5)。机械通气的中位持续时间为5.8天(IQR,3.1至11.4)。35例患者在入院后48小时内有AKI证据,其中24例(69%)在进入ICU时就已经有AKI。AKI患者中uNGAL和KIM-1浓度分别在入院后6至12小时和12至24小时达到峰值。入院后0至6小时,uNGAL的最大受试者工作特征曲线下面积(AUC)为0.815(95%置信区间(CI),0.685至0.945,P<0.001)。KIM-1的鉴别能力中等,入院后12至24小时最大AUC为0.737(95%CI,0.628至0.847;P<0.001)。在最佳截断点(126 ng/ml)时,uNGAL浓度在19名儿童中的16名(84%)中正确预测了AKI的发生,比SCr升高明显提前24小时。
入住ICU后发生AKI的患者中uNGAL和KIM-1水平升高,分别在入院后6至12小时和12至24小时达到峰值。uNGAL似乎是识别24小时后将发生AKI儿童的可靠标志物。