Akiyama Eiichi, Cinotti Raphaël, Čerlinskaitė Kamilė, Van Aelst Lucas N L, Arrigo Mattia, Placido Rui, Chouihed Tahar, Girerd Nicolas, Zannad Faiez, Rossignol Patrick, Badoz Marc, Launay Jean-Marie, Gayat Etienne, Cohen-Solal Alain, Lam Carolyn S P, Testani Jeffrey, Mullens Wilfried, Cotter Gad, Seronde Marie-France, Mebazaa Alexandre
Inserm UMR-S 942, Paris, France.
Division of Cardiology, Yokohama City University Medical Center, Yokohama, Japan.
ESC Heart Fail. 2020 Jun;7(3):996-1006. doi: 10.1002/ehf2.12645. Epub 2020 Apr 11.
Changes in echocardiographic parameters and biomarkers of cardiac and venous pressures or estimated plasma volume during hospitalization associated with decongestive treatments in acute heart failure (AHF) patients with either preserved left ventricular ejection fraction (LVEF) (HFPEF) or reduced LVEF (HFREF) are poorly assessed.
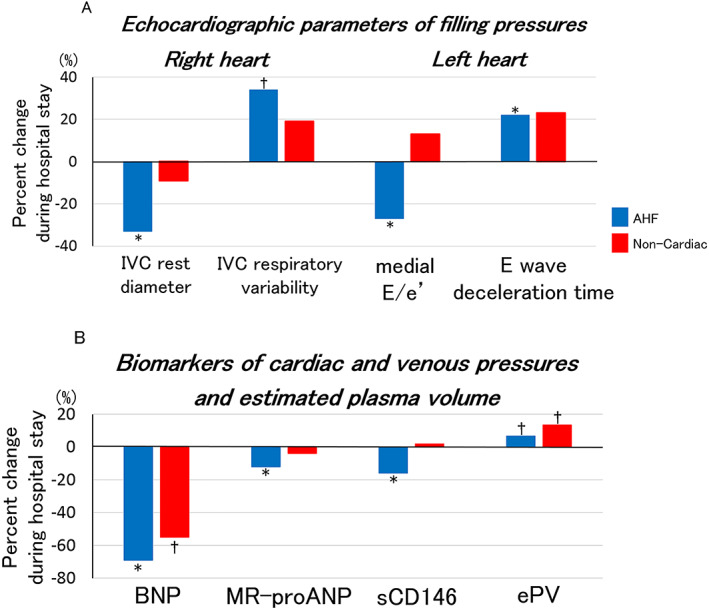
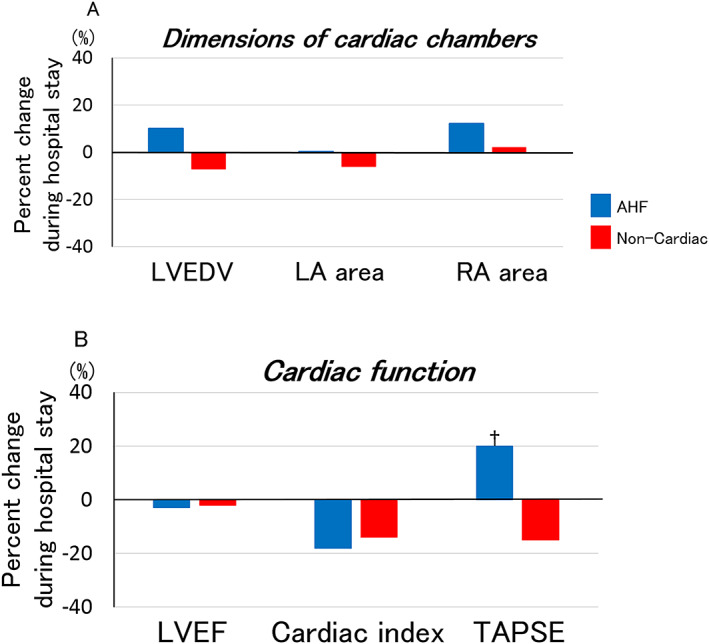
From the metabolic road to diastolic heart failure: diastolic heart failure (MEDIA-DHF) study, 111 patients were included in this substudy: 77 AHF (43 HFPEF and 34 HFREF) and 34 non-cardiac dyspnea patients. Echocardiographic measurements and blood samples were obtained within 4 h of presentation at the emergency department and before hospital discharge. In AHF patients, echocardiographic indices of cardiac and venous pressures, including inferior vena cava diameter [from 22 (16-24) mm to 13 (11-18) mm, P = 0.009], its respiratory variability [from 32 (8-44) % to 43 (29-70) %, P = 0.04], medial E/e' [from 21.1 (15.8-29.6) to 16.6 (11.7-24.3), P = 0.004], and E wave deceleration time [from 129 (105-156) ms to 166 (128-203) ms, P = 0.003], improved during hospitalization, similarly in HFPEF and HFREF patients. By contrast, no changes were seen in non-cardiac dyspnea patients. In AHF patients, all plasma biomarkers of cardiac and venous pressures, namely B-type natriuretic peptide [from 935 (514-2037) pg/mL to 308 (183-609) pg/mL, P < 0.001], mid-regional pro-atrial natriuretic peptide [from 449 (274-653) pmol/L to 366 (242-549) pmol/L, P < 0.001], and soluble CD-146 levels [from 528 (406-654) ng/mL to 450 (374-529) ng/mL, P = 0.003], significantly decreased during hospitalization, similarly in HFPEF and HFREF patients. Echocardiographic parameters of cardiac chamber dimensions [left ventricular end-diastolic volume: from 120 (76-140) mL to 118 (95-176) mL, P = 0.23] and cardiac index [from 2.1 (1.6-2.6) mL/min/m to 1.9 (1.4-2.4) mL/min/m , P = 0.55] were unchanged in AHF patients, except tricuspid annular plane systolic excursion (TAPSE) that improved during hospitalization [from 16 (15-19) mm to 19 (17-21) mm, P = 0.04]. Estimated plasma volume increased in both AHF [from 4.8 (4.2-5.6) to 5.1 (4.4-5.8), P = 0.03] and non-cardiac dyspnea patients (P = 0.01). Serum creatinine [from 1.18 (0.90-1.53) to 1.19 (0.86-1.70) mg/dL, P = 0.89] and creatinine-based estimated glomerular filtration rate [from 59 (40-75) mL/min/1.73m to 56 (38-73) mL/min/1.73m , P = 0.09] were similar, while plasma cystatin C [from 1.50 (1.20-2.27) mg/L to 1.78 (1.33-2.59) mg/L, P < 0.001] and neutrophil gelatinase associated lipocalin (NGAL) [from 127 (95-260) ng/mL to 167 (104-263) ng/mL, P = 0.004] increased during hospitalization in AHF.
Echocardiographic parameters and plasma biomarkers of cardiac and venous pressures improved during AHF hospitalization in both acute HFPEF and HFREF patients, while cardiac chamber dimensions, cardiac output, and estimated plasma volume showed minimal changes.
对于射血分数保留(HFPEF)或射血分数降低(HFREF)的急性心力衰竭(AHF)患者,在住院期间与去充血治疗相关的超声心动图参数以及心脏和静脉压力生物标志物或估计血浆量的变化评估不足。
来自“从代谢途径到舒张性心力衰竭:舒张性心力衰竭(MEDIA - DHF)”研究,111例患者纳入本亚研究:77例AHF患者(43例HFPEF和34例HFREF)以及34例非心源性呼吸困难患者。在急诊科就诊后4小时内及出院前获取超声心动图测量值和血样。在AHF患者中,心脏和静脉压力的超声心动图指标,包括下腔静脉直径[从22(16 - 24)mm至13(11 - 18)mm,P = 0.009]、其呼吸变异性[从32(8 - 44)%至43(29 - 70)%,P = 0.04]、E/e'平均值[从21.1(15.8 - 29.6)至16.6(11.7 - 24.3),P = 0.004]以及E波减速时间[从129(105 - 156)ms至166(128 - 203)ms,P = 0.003]在住院期间均有改善,HFPEF和HFREF患者情况相似。相比之下,非心源性呼吸困难患者未见变化。在AHF患者中,所有心脏和静脉压力的血浆生物标志物,即B型利钠肽[从935(514 - 2037)pg/mL至308(183 - 609)pg/mL,P < 0.001]、中段心房利钠肽原[从449(274 - 653)pmol/L至366(242 - 549)pmol/L,P < 0.001]以及可溶性CD - 146水平[从528(406 - 654)ng/mL至450(374 - 529)ng/mL,P = 0.003]在住院期间均显著降低,HFPEF和HFREF患者情况相似。AHF患者中心腔尺寸的超声心动图参数[左心室舒张末期容积:从120(76 - 140)mL至118(95 - 176)mL,P = 0.23]和心脏指数[从2.1(1.6 - 2.6)mL/min/m至1.9(1.4 - 2.4)mL/min/m ,P = 0.55]无变化,但三尖瓣环平面收缩期位移(TAPSE)在住院期间有所改善[从16(15 - 19)mm至19(17 - 21)mm,P = 0.04]。AHF患者和非心源性呼吸困难患者的估计血浆量均增加[AHF患者从4.8(4.2 - 5.6)至5.1(4.4 - 5.8),P = 0.03;非心源性呼吸困难患者P = 0.01]。血清肌酐[从1.18(0.90 - 1.53)至1.19(0.86 - 1.70)mg/dL,P = 0.89]和基于肌酐的估计肾小球滤过率[从59(40 - 75)mL/min/1.73m至56(38 - 73)mL/min/1.73m ,P = 0.09]相似,而AHF患者住院期间血浆胱抑素C[从1.50(1.20 - 2.27)mg/L至1.78(1.33 - 2.59)mg/L,P < 0.001]和中性粒细胞明胶酶相关脂质运载蛋白(NGAL)[从127(95 - 260)ng/mL至167(104 - 263)ng/mL,P = 0.004]升高。
在急性HFPEF和HFREF患者的AHF住院期间,心脏和静脉压力的超声心动图参数及血浆生物标志物有所改善,而心腔尺寸、心输出量和估计血浆量变化极小。