Monterde David, Cainzos-Achirica Miguel, Cossio-Gil Yolima, García-Eroles Luis, Pérez-Sust Pol, Arrufat Miquel, Calle Candela, Comin-Colet Josep, Velasco César
Catalan Institute of Health, Barcelona, Spain.
Johns Hopkins Ciccarone Center for the Prevention of Cardiovascular Disease, Johns Hopkins Medical Institutions, Baltimore, MD, USA.
Risk Manag Healthc Policy. 2020 Mar 26;13:271-283. doi: 10.2147/RMHP.S228415. eCollection 2020.
Accurate risk adjustment is crucial for healthcare management and benchmarking.
We aimed to compare the performance of classic comorbidity functions (Charlson's and Elixhauser's), of the All Patients Refined Diagnosis Related Groups (APR-DRG), and of the Queralt Indices, a family of novel, comprehensive comorbidity indices for the prediction of key clinical outcomes in hospitalized patients.
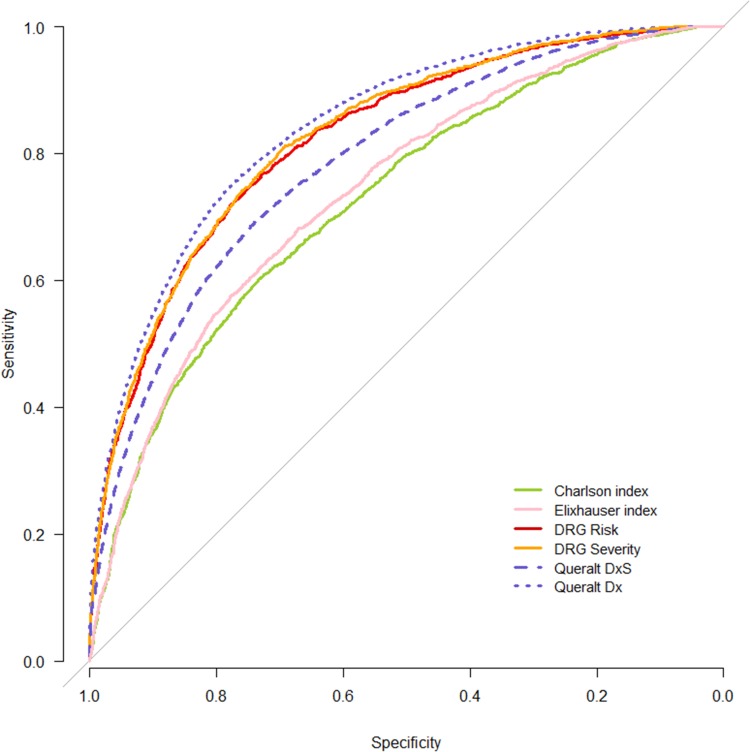
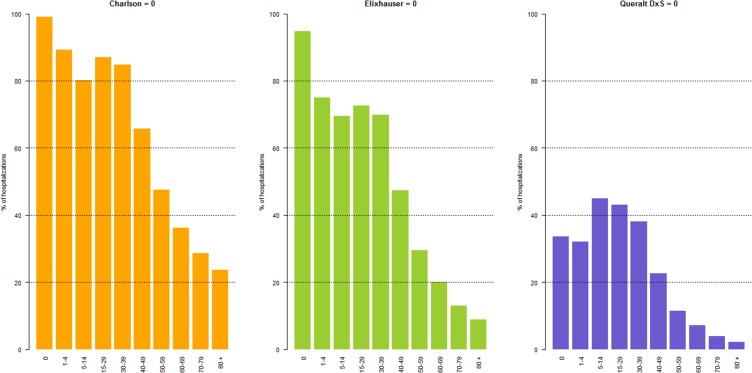
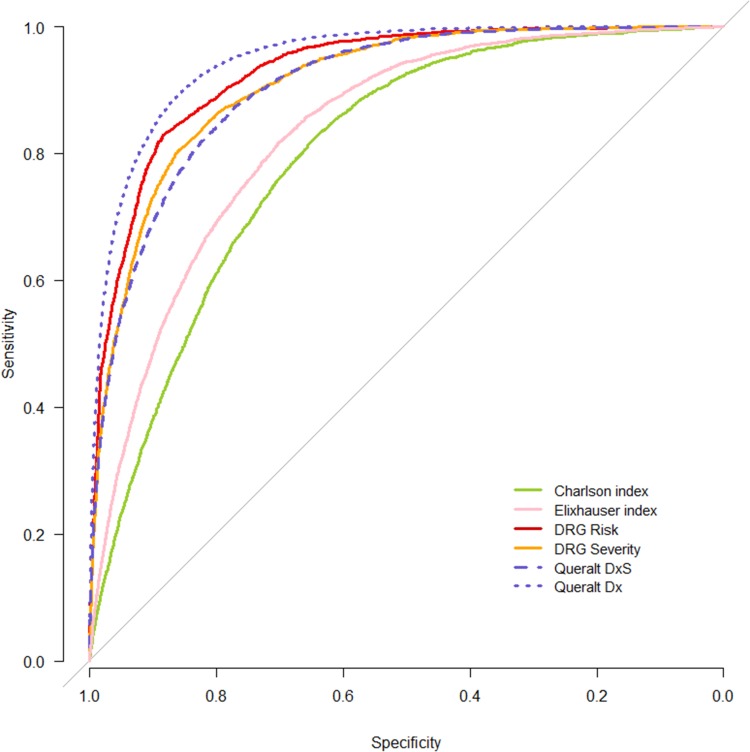
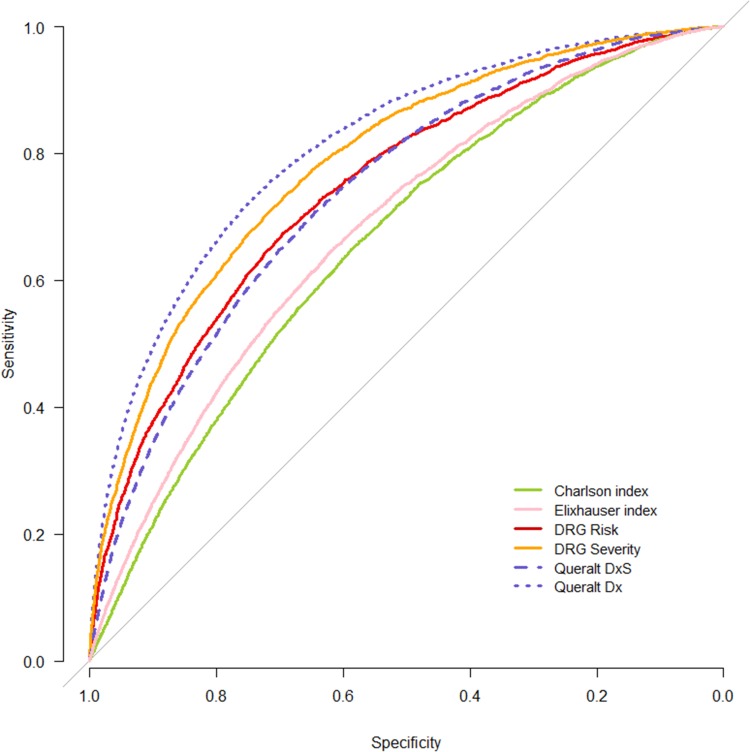
We conducted an observational, retrospective cohort study using administrative healthcare data from 156,459 hospital discharges in Catalonia (Spain) during 2018. Study outcomes were in-hospital death, long hospital stay, and intensive care unit (ICU) stay. We evaluated the performance of the following indices: Charlson's and Elixhauser's functions, Queralt's Index for secondary hospital discharge diagnoses (Queralt DxS), the overall Queralt's Index, which includes pre-existing comorbidities, in-hospital complications, and principal discharge diagnosis (Queralt Dx), and the APR-DRG. Discriminative ability was evaluated using the area under the curve (AUC), and measures of goodness of fit were also computed. Subgroup analyses were conducted by principal discharge diagnosis, by age, and type of admission.
Queralt DxS provided relevant risk adjustment information in a larger number of patients compared to Charlson's and Elixhauser's functions, and outperformed both for the prediction of the 3 study outcomes. Queralt Dx also outperformed Charlson's and Elixhauser's indices, and yielded superior predictive ability and goodness of fit compared to APR-DRG (AUC for in-hospital death 0.95 for Queralt Dx, 0.77-0.93 for all other indices; for ICU stay 0.84 for Queralt Dx, 0.73-0.83 for all other indices). The performance of Queralt DxS was at least as good as that of the APR-DRG in most principal discharge diagnosis subgroups.
Our findings suggest that risk adjustment should go beyond pre-existing comorbidities and include principal discharge diagnoses and in-hospital complications. Validation of comprehensive risk adjustment tools such as the Queralt indices in other settings is needed.
准确的风险调整对于医疗管理和基准化至关重要。
我们旨在比较经典共病函数(查尔森和埃利克斯豪泽的函数)、所有患者精细诊断相关组(APR-DRG)以及夸拉特指数(一组用于预测住院患者关键临床结局的新型综合共病指数)的性能。
我们利用2018年西班牙加泰罗尼亚地区156459例医院出院的行政医疗数据进行了一项观察性回顾性队列研究。研究结局为住院死亡、住院时间延长和重症监护病房(ICU)住院时间。我们评估了以下指数的性能:查尔森和埃利克斯豪泽的函数、夸拉特二级医院出院诊断指数(夸拉特DxS)、包括既往共病、住院并发症和主要出院诊断的总体夸拉特指数(夸拉特Dx)以及APR-DRG。使用曲线下面积(AUC)评估判别能力,并计算拟合优度指标。按主要出院诊断、年龄和入院类型进行亚组分析。
与查尔森和埃利克斯豪泽的函数相比,夸拉特DxS在更多患者中提供了相关的风险调整信息,并且在预测3项研究结局方面均优于二者。夸拉特Dx也优于查尔森和埃利克斯豪泽的指数,并且与APR-DRG相比具有更高的预测能力和拟合优度(夸拉特Dx的住院死亡AUC为0.95,所有其他指数为0.77 - 0.93;ICU住院时间夸拉特Dx为0.84,所有其他指数为0.73 - 0.83)。在大多数主要出院诊断亚组中,夸拉特DxS的性能至少与APR-DRG一样好。
我们的研究结果表明,风险调整应超越既往共病,纳入主要出院诊断和住院并发症。需要在其他环境中验证诸如夸拉特指数等综合风险调整工具。