Hospital Clínic de Barcelona, Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Universitat de Barcelona, Barcelona, Spain.
Consorci d'Atenció Primària de Salut Barcelona Esquerra (CAPSBE), Primary Healthcare Transversal Research Group, Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain.
J Med Internet Res. 2023 Feb 16;25:e40846. doi: 10.2196/40846.
Enhanced management of multimorbidity constitutes a major clinical challenge. Multimorbidity shows well-established causal relationships with the high use of health care resources and, specifically, with unplanned hospital admissions. Enhanced patient stratification is vital for achieving effectiveness through personalized postdischarge service selection.
The study has a 2-fold aim: (1) generation and assessment of predictive models of mortality and readmission at 90 days after discharge; and (2) characterization of patients' profiles for personalized service selection purposes.
Gradient boosting techniques were used to generate predictive models based on multisource data (registries, clinical/functional and social support) from 761 nonsurgical patients admitted in a tertiary hospital over 12 months (October 2017 to November 2018). K-means clustering was used to characterize patient profiles.
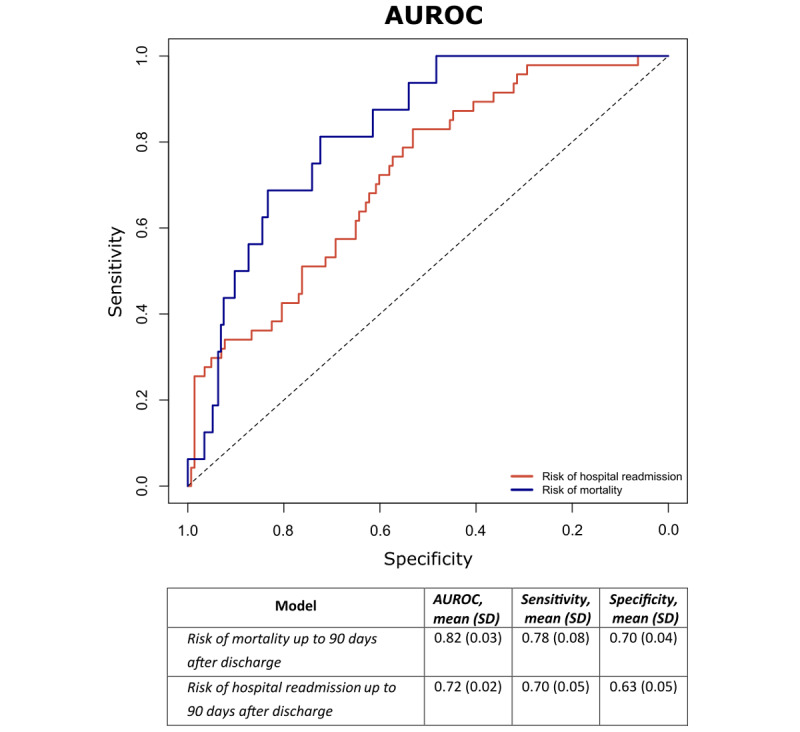
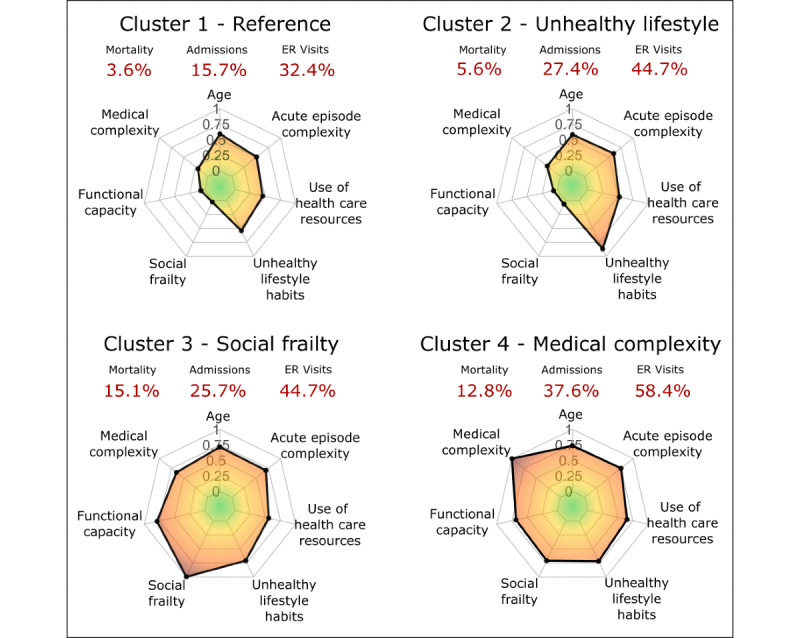
Performance (area under the receiver operating characteristic curve, sensitivity, and specificity) of the predictive models was 0.82, 0.78, and 0.70 and 0.72, 0.70, and 0.63 for mortality and readmissions, respectively. A total of 4 patients' profiles were identified. In brief, the reference patients (cluster 1; 281/761, 36.9%), 53.7% (151/281) men and mean age of 71 (SD 16) years, showed 3.6% (10/281) mortality and 15.7% (44/281) readmissions at 90 days following discharge. The unhealthy lifestyle habit profile (cluster 2; 179/761, 23.5%) predominantly comprised males (137/179, 76.5%) with similar age, mean 70 (SD 13) years, but showed slightly higher mortality (10/179, 5.6%) and markedly higher readmission rate (49/179, 27.4%). Patients in the frailty profile (cluster 3; 152/761, 19.9%) were older (mean 81 years, SD 13 years) and predominantly female (63/152, 41.4%, males). They showed medical complexity with a high level of social vulnerability and the highest mortality rate (23/152, 15.1%), but with a similar hospitalization rate (39/152, 25.7%) compared with cluster 2. Finally, the medical complexity profile (cluster 4; 149/761, 19.6%), mean age 83 (SD 9) years, 55.7% (83/149) males, showed the highest clinical complexity resulting in 12.8% (19/149) mortality and the highest readmission rate (56/149, 37.6%).
The results indicated the potential to predict mortality and morbidity-related adverse events leading to unplanned hospital readmissions. The resulting patient profiles fostered recommendations for personalized service selection with the capacity for value generation.
对多种疾病的强化管理是一项重大的临床挑战。多种疾病与医疗资源的大量使用有着明确的因果关系,特别是与非计划性住院有关。为了通过个性化的出院后服务选择实现效果,对患者进行分层至关重要。
本研究有两个目的:(1)生成和评估出院后 90 天内死亡率和再入院率的预测模型;(2)为个性化服务选择目的对患者特征进行分类。
使用梯度提升技术基于 761 名非手术患者的多源数据(来自登记处、临床/功能和社会支持)生成预测模型,这些患者在一家三级医院住院 12 个月(2017 年 10 月至 2018 年 11 月)。使用 K-均值聚类对患者特征进行分类。
预测模型的性能(接收者操作特征曲线下的面积、敏感性和特异性)为 0.82、0.78 和 0.70 以及 0.72、0.70 和 0.63 分别用于死亡率和再入院率。共确定了 4 种患者特征。简而言之,参考患者(第 1 组;761 例患者中的 281 例,36.9%),53.7%(281 例中的 151 例)为男性,平均年龄为 71 岁(标准差为 16 岁),出院后 90 天的死亡率为 3.6%(281 例中的 10 例),再入院率为 15.7%(281 例中的 44 例)。不健康生活方式习惯特征(第 2 组;761 例患者中的 179 例,23.5%)主要由男性(179 例中的 137 例,76.5%)组成,年龄相似,平均为 70 岁(标准差为 13 岁),但死亡率略高(179 例中的 10 例,5.6%),再入院率明显更高(179 例中的 49 例,27.4%)。衰弱特征患者(第 3 组;761 例患者中的 152 例,19.9%)年龄较大(平均 81 岁,标准差 13 岁),主要为女性(152 例中的 63 例,41.4%,男性)。他们表现出较高的医疗复杂性,具有较高的社会脆弱性,死亡率最高(152 例中的 23 例,15.1%),但与第 2 组相比,住院率相似(152 例中的 39 例,25.7%)。最后,医疗复杂性特征(第 4 组;761 例患者中的 149 例,19.6%),平均年龄 83 岁(标准差 9 岁),55.7%(149 例中的 83 例)为男性,表现出最高的临床复杂性,导致 12.8%(149 例中的 19 例)的死亡率和最高的再入院率(149 例中的 56 例,37.6%)。
结果表明有可能预测导致非计划性住院再入院的死亡率和发病率相关不良事件。由此产生的患者特征促进了个性化服务选择的建议,具有产生价值的能力。