Ling Diane C, Iarrobino Nick A, Champ Colin E, Soran Atilla, Beriwal Sushil
Department of Radiation Oncology, University of Pittsburgh Medical Center Hillman Cancer Center, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania.
Breast Surgery Unit, Department of Surgical Oncology, University of Pittsburgh Medical Center Magee-Women's Hospital, Pittsburgh, Pennsylvania.
Adv Radiat Oncol. 2019 Sep 27;5(2):163-170. doi: 10.1016/j.adro.2019.09.006. eCollection 2020 Mar-Apr.
Current standard of care for patients with breast cancer with a positive node on sentinel lymph node biopsy (SLNB) after neoadjuvant chemotherapy is axillary dissection with irradiation of the regional nodes, but it is unknown whether axillary lymph node dissection (ALND) can be safely omitted if complete axillary radiation is delivered instead.
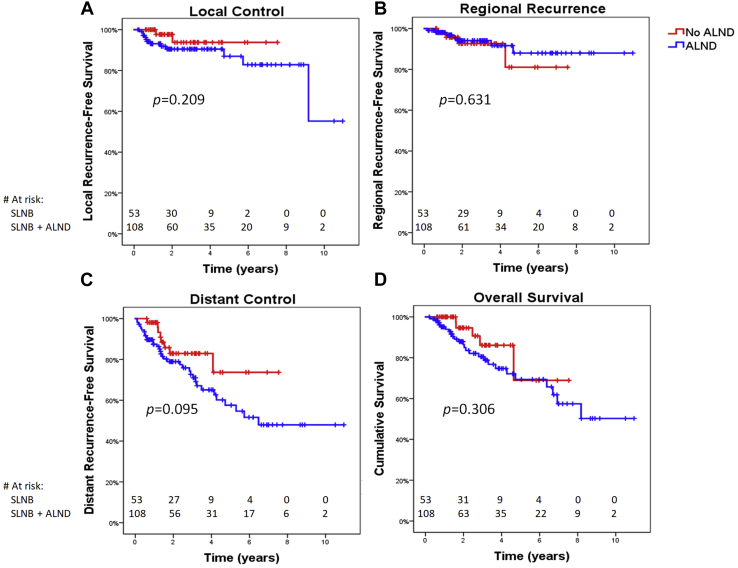
We identified 161 patients found to have a positive sentinel lymph node on SLNB after neoadjuvant chemotherapy for breast cancer between December 2006 and October 2017, who were treated with or without completion ALND. Local, regional, and distant recurrence and overall survival were analyzed using the Kaplan-Meier method. Patient, disease, and treatment factors potentially predictive of each outcome were entered into Cox regression analysis.
Median follow-up was 28.8 months (range, 2.5-137.0). The 3-year regional control rate did not differ according to extent of axillary surgery (92.6% for SLNB alone vs 96.4% for SLNB with ALND, = .616). Regional recurrence occurred as part of first recurrence in 9 patients (5.6%). Five patients failed in axillary levels 1 or 2, 6 failed in axillary level 3 or supraclavicular nodes, and 2 failed in internal mammary nodes, with some patients failing in multiple regional nodal areas. Extent of axillary dissection (SLNB only vs SLNB plus ALND) did not predict for disease control or survival. Patients who underwent ALND were significantly more likely to have lymphedema (25.0% vs 9.4%, = .021).
Careful selection of patients with a positive sentinel node on SLNB after neoadjuvant chemotherapy for omission of completion ALND in favor of irradiation of the undissected axilla does not compromise local, regional, or distant control or overall survival and results in lower rates of lymphedema.
新辅助化疗后前哨淋巴结活检(SLNB)显示淋巴结阳性的乳腺癌患者,当前的标准治疗方案是腋窝清扫并对区域淋巴结进行放射治疗,但如果改为进行全腋窝放疗,是否可以安全地省略腋窝淋巴结清扫(ALND)尚不清楚。
我们确定了2006年12月至2017年10月期间新辅助化疗后经SLNB发现前哨淋巴结阳性的161例乳腺癌患者,这些患者接受或未接受完整的ALND治疗。采用Kaplan-Meier方法分析局部、区域和远处复发情况以及总生存率。将可能预测每种结局的患者、疾病和治疗因素纳入Cox回归分析。
中位随访时间为28.8个月(范围2.5 - 137.0个月)。腋窝手术范围不同,3年区域控制率无差异(单纯SLNB为92.6%,SLNB联合ALND为96.4%,P = 0.616)。9例患者(5.6%)出现区域复发,为首次复发的一部分。5例患者腋窝1或2级淋巴结转移失败,6例患者腋窝3级或锁骨上淋巴结转移失败,2例患者内乳淋巴结转移失败,部分患者在多个区域淋巴结区域转移失败。腋窝清扫范围(仅SLNB与SLNB加ALND)不能预测疾病控制或生存情况。接受ALND的患者发生淋巴水肿的可能性显著更高(25.0%对9.4%,P = 0.021)。
对于新辅助化疗后SLNB显示前哨淋巴结阳性的患者,谨慎选择省略完整的ALND而改为对未清扫的腋窝进行放疗,不会影响局部、区域或远处控制或总生存率,且淋巴水肿发生率较低。