University of Miami, Miller School of Medicine, Miami, FL, USA.
DeWitt Daughtry Family Department of Surgery, University of Miami Miller School of Medicine, Miami, FL, USA.
World J Surg Oncol. 2024 Jul 29;22(1):199. doi: 10.1186/s12957-024-03477-4.
Low false negative rates can be achieved with sentinel lymph node biopsy (SLNB) after neoadjuvant chemotherapy (NAC) in breast cancer (BC) patients with clinical N1 (cN1) disease. We examined changes in axillary management and oncologic outcomes in BC patients with cN1 disease receiving NAC.
BC patients with biopsy proven cN1 disease treated with NAC were selected from our institutional cancer registry (2014-2017). Patients were grouped by axillary management, axillary lymph node dissection (ALND), SLNB followed by ALND, or SLNB alone. Univariable and multivariable survival analysis for recurrence-free survival (RFS) and overall survival (OS) were performed.
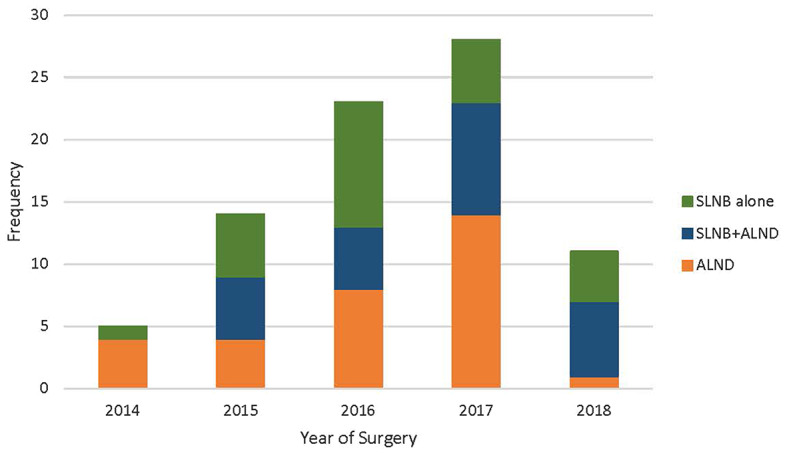
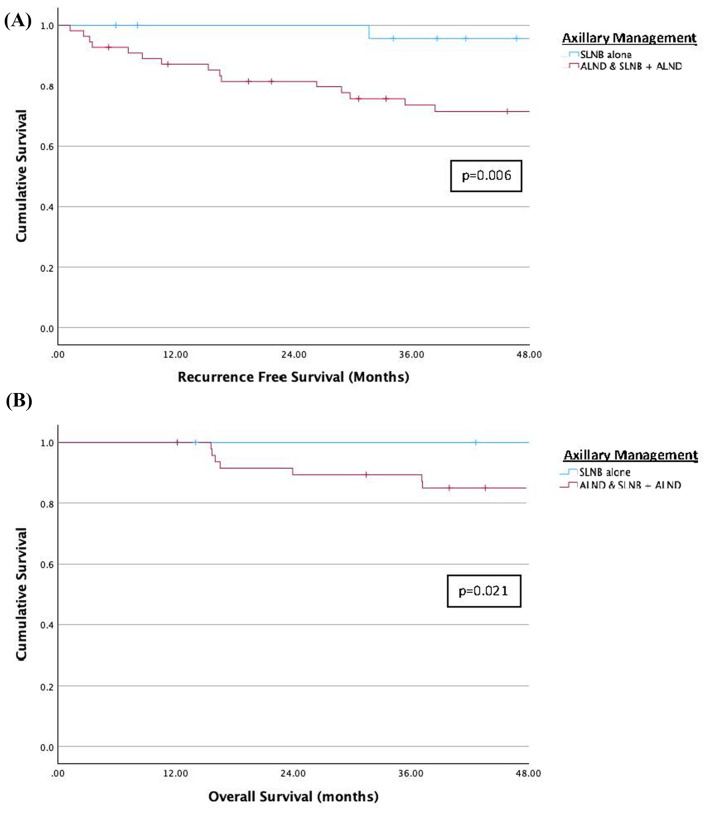
81 patients met inclusion criteria: 31 (38%) underwent ALND, 25 (31%) SLNB + ALND, and 25 (31%) SLNB alone. A SLN was identified in 45/50 (90%) patients who had SLNB. ALND was performed in 25/50 (50%) patients who had SLNB: 18 for a + SLNB, 5 failed SLNB, and 2 insufficient SLNs. 25 patients had SLNB alone, 17 were SLN- and 8 SLN+. In the SLNB alone group, 23/25 (92%) patients received adjuvant radiation (RT). 20 (25%) patients developed BC recurrence: 14 distant (70%), 3 local (15%), 2 regional + distant (10%), and 1 contralateral (5%). In the SLNB alone group, there was 1 axillary recurrence in a patient with a negative SLNB who did not receive RT. Univariable survival analysis showed significant differences in RFS and OS between axillary management groups, ALND/SLNB + ALND vs. SLNB alone (RFS: p = 0.006, OS: p = 0.021). On multivariable survival analysis, worse RFS and OS were observed in patients with TNBC (RFS: HR 3.77, 95% CI 1.70-11.90, p = 0.023; OS: HR 8.10, 95% CI 1.84-35.60, p = 0.006).
SLNB alone and RT after NAC in BC patients with cN1 disease who have negative SLNs at surgery provides long-term regional disease control. This analysis provides support for the practice of axillary downstaging with NAC and SLNB alone.
新辅助化疗(NAC)后,临床 N1(cN1)期乳腺癌患者行前哨淋巴结活检(SLNB)可获得较低的假阴性率。我们检测了接受 NAC 的 cN1 期乳腺癌患者腋窝管理和肿瘤学结局的变化。
从我们的机构癌症登记处选择经活检证实为 cN1 疾病且接受 NAC 治疗的乳腺癌患者(2014-2017 年)。根据腋窝管理方式将患者分为腋窝淋巴结清扫术(ALND)组、SLNB 后 ALND 组或 SLNB 单独组。对无复发生存率(RFS)和总生存(OS)进行单变量和多变量生存分析。
81 例患者符合纳入标准:31 例(38%)行 ALND,25 例(31%)行 SLNB+ALND,25 例(31%)行 SLNB 单独组。50 例行 SLNB 的患者中有 45 例(90%)识别出了前哨淋巴结。25 例行 SLNB 的患者中,有 25 例行 ALND:18 例为阳性 SLNB,5 例为 SLNB 失败,2 例为 SLN 不足。25 例患者行 SLNB 单独组,17 例为 SLN-,8 例为 SLN+。在 SLNB 单独组中,23/25(92%)例患者接受了辅助放疗(RT)。20 例(25%)患者发生乳腺癌复发:14 例远处转移(70%),3 例局部转移(15%),2 例区域+远处转移(10%),1 例对侧(5%)。在 SLNB 单独组中,1 例阴性 SLNB 患者未接受 RT,出现 1 例腋窝复发。单变量生存分析显示,腋窝管理组之间的 RFS 和 OS 差异有统计学意义,ALND/SLNB+ALND 与 SLNB 单独组相比(RFS:p=0.006,OS:p=0.021)。多变量生存分析显示,三阴性乳腺癌(TNBC)患者的 RFS 和 OS 较差(RFS:HR 3.77,95%CI 1.70-11.90,p=0.023;OS:HR 8.10,95%CI 1.84-35.60,p=0.006)。
cN1 期乳腺癌患者在新辅助化疗后行 SLNB 单独和 SLNB 术后阴性的腋窝淋巴结清扫术,可提供长期的区域疾病控制。该分析为 NAC 后行腋窝降期和 SLNB 单独治疗的临床实践提供了支持。