Kearsley-Fleet Lianne, Heaf Eleanor, Davies Rebecca, Baildam Eileen, Beresford Michael W, Foster Helen E, Southwood Taunton R, Thomson Wendy, Hyrich Kimme L
Centre for Epidemiology Versus Arthritis, The University of Manchester, Manchester Academic Health Science Centre, Manchester, UK.
Clinical Academic Department of Paediatric Rheumatology, Alder Hey Children's NHS Foundation Trust, Liverpool, UK.
Lancet Rheumatol. 2020 Mar 9;2(4):e217-e226. doi: 10.1016/S2665-9913(20)30025-4. eCollection 2020 Apr.
Information is scarce about biological disease-modifying antirheumatic drug (DMARD) switching patterns in children and young people (aged ≤16 years) with juvenile idiopathic arthritis in an era of many biologic therapies. The best choice of biologic to use if the first biological DMARD is not beneficial also remains unclear. We aimed to quantify and characterise biologic switching patterns in children and young people with juvenile idiopathic arthritis, and to compare the effectiveness of using a second tumour necrosis factor inhibitor (TNFi) versus non-TNF is following failure of a first TNFi biologic in routine clinical practice.
Our study population comprised patients with juvenile idiopathic arthritis who were enrolled in two parallel UK cohort studies (the British Society for Paediatric and Adolescent Rheumatology Etanercept Cohort Study [BSPAR-ETN] and the Biologics for Children with Rheumatic Diseases [BCRD] study) between Jan 1, 2004, and April 11, 2019. Data on disease characteristics and DMARD therapy were collected at the time of initiation of a first biologic, at 6 months, at 1 year, and annually thereafter. Biologic switching patterns were described in all patients who started their first biologic from Jan 1, 2010, onwards. Among patients who started treatment with their first biologic from Jan 1, 2004, onwards, had polyarticular course juvenile idiopathic arthritis (extended oligoarthritis or polyarthritis [positive or negative for rheumatoid factor]), and who had started a second biologic, we assessed changes in outcome variables at 6 months compared with baseline and compared the proportion of patients who achieved an American College of Rheumatology Pediatric (ACR Pedi) 90 response and minimal disease activity at 6 months on the basis of the class of the second biologic (a second TNFi non-TNFi biologic). Changes in outcome variables at 6 months were compared using linear regression or logistic regression, adjusted for propensity quintiles to account for confounding by indication. We used multiple imputation to account for missing data.
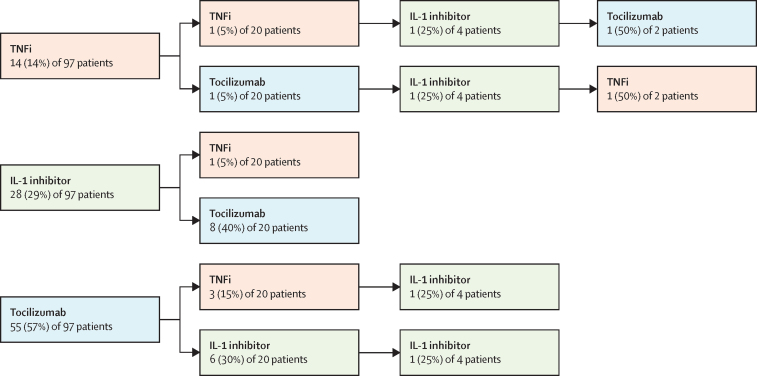
Between Jan 1, 2004, and April 11, 2019, 2361 patients were enrolled on initiation of biologic therapy. From Jan 1, 2010, onwards, 1152 patients started their first biologic, most of whom started treatment with TNFis (1050 [91%]). The median follow-up was 2·2 years (IQR 1·1-3·8). During this time, 270 (23%) of 1152 patients started a second biologic, 61 (5%) started a third biologic, and 11 (1%) started a fourth biologic. Among 240 patients with polyarticular-course juvenile idiopathic arthritis, 194 (81%) started a second TNFi and 46 (19%) started a non-TNFi after an initial TNFi had failed. Choice of second treatment (second TNFi non-TNFi biologic) did not affect the proportion of patients who achieved an ACR Pedi 90 response (adjusted odds ratio [OR] 2·5, 95% CI 0·8-7·9; p=0·11) or minimal disease activity (adjusted OR 1·6, 95% CI 0·6-3·8; p=0·33).
For many children and young people with juvenile idiopathic arthritis, treatment with a first or second biologic is not beneficial. We found no evidence that switching to a second non-TNFi biologic was more beneficial than a second TNFi.
Versus Arthritis and The British Society for Rheumatology.
在生物疗法众多的时代,关于儿童和青少年(年龄≤16岁)幼年特发性关节炎患者使用改善病情抗风湿生物药(DMARD)的换药模式的信息匮乏。如果第一种生物DMARD无效,最佳的生物药选择仍不明确。我们旨在量化并描述幼年特发性关节炎儿童和青少年的生物药换药模式,并比较在常规临床实践中,第一种肿瘤坏死因子抑制剂(TNFi)生物药治疗失败后,使用第二种TNFi与非TNFi生物药的有效性。
我们的研究人群包括在2004年1月1日至2019年4月11日期间纳入两项平行英国队列研究(英国儿科学会和青少年风湿病学会依那西普队列研究 [BSPAR - ETN] 和风湿病患儿生物制剂 [BCRD] 研究)的幼年特发性关节炎患者。在开始使用第一种生物药时、6个月时、1年时以及此后每年收集疾病特征和DMARD治疗数据。描述了从2010年1月1日起开始使用第一种生物药的所有患者的生物药换药模式。在2004年1月1日起开始使用第一种生物药、患有多关节型幼年特发性关节炎(扩展性寡关节炎或多关节炎 [类风湿因子阳性或阴性])且开始使用第二种生物药的患者中,我们评估了6个月时与基线相比结局变量的变化,并根据第二种生物药的类别(第二种TNFi或非TNFi生物药)比较了6个月时达到美国风湿病学会儿科(ACR Pedi)90反应和最小疾病活动度的患者比例。使用线性回归或逻辑回归比较6个月时结局变量的变化,并根据倾向五分位数进行调整以考虑适应证的混杂因素。我们使用多重填补法处理缺失数据。
在2004年1月1日至2019年4月11日期间,2361例患者开始接受生物治疗。从2010年1月1日起,1152例患者开始使用第一种生物药,其中大多数开始使用TNFi(1050例 [91%])。中位随访时间为2.2年(IQR 1.1 - 3.8)。在此期间,1152例患者中有270例(23%)开始使用第二种生物药,61例(5%)开始使用第三种生物药,11例(1%)开始使用第四种生物药。在240例多关节型幼年特发性关节炎患者中,194例(81%)在初始TNFi治疗失败后开始使用第二种TNFi,46例(19%)开始使用非TNFi。第二种治疗的选择(第二种TNFi或非TNFi生物药)不影响达到ACR Pedi 90反应的患者比例(调整后的优势比 [OR] 为2.5,95% CI 0.8 - 7.9;p = 0.11)或最小疾病活动度(调整后的OR为1.6,95% CI 0.6 - 3.8;p = 0.33)。
对于许多幼年特发性关节炎儿童和青少年,使用第一种或第二种生物药治疗并无益处。我们没有发现证据表明换用第二种非TNFi生物药比第二种TNFi更有益。
关节炎对抗组织和英国风湿病学会。