Stroke Research Group, Institute of Neuroscience, Newcastle University, Newcastle upon Tyne, United Kingdom.
Swansea University Medical School, Swansea, Wales, United Kingdom.
JAMA Neurol. 2020 Jul 1;77(7):840-848. doi: 10.1001/jamaneurol.2020.0611.
Rapid thrombolysis treatment for acute ischemic stroke reduces disability among patients who are carefully selected, but service delivery is challenging.
To determine whether an enhanced Paramedic Acute Stroke Treatment Assessment (PASTA) intervention increased hospital thrombolysis rates.
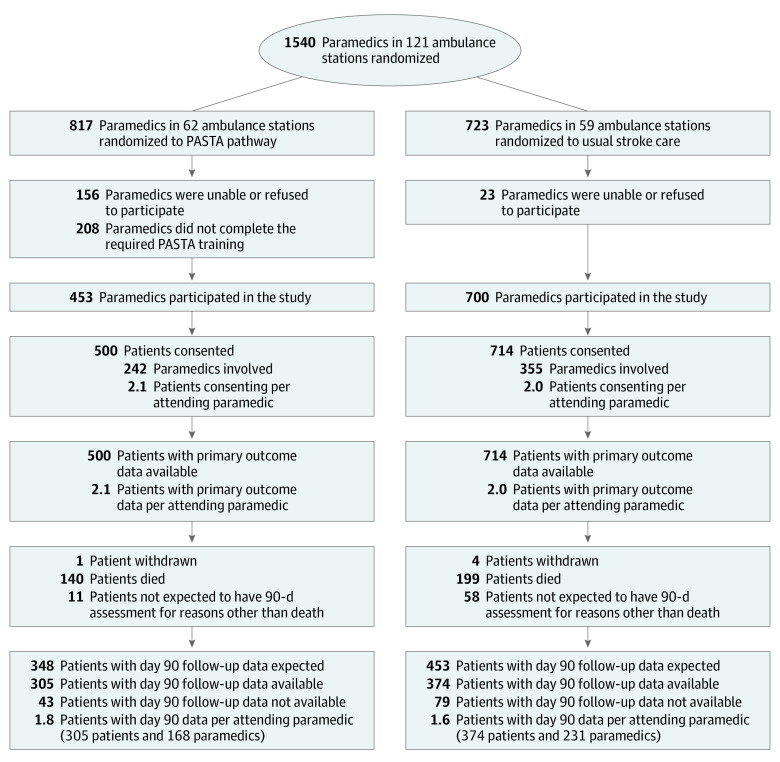
DESIGN, SETTING, AND PARTICIPANTS: This multicenter, cluster randomized clinical trial took place between December 2015 and July 2018 in 3 ambulance services and 15 hospitals. Clusters were paramedics based within ambulance stations prerandomized to PASTA or standard care. Patients attended by study paramedics were enrolled after admission if a hospital specialist confirmed a stroke and paramedic assessment started within 4 hours of onset. Allocation to PASTA or standard care reflected the attending paramedic's randomization status.
The PASTA intervention included additional prehospital information collection, a structured hospital handover, practical assistance up to 15 minutes after handover, a predeparture care checklist, and clinician feedback. Standard care reflected national guidelines.
Primary outcome was the proportion of patients receiving thrombolysis. Secondary outcomes included time intervals and day 90 health (with poor status defined as a modified Rankin Score >2, to represent dependency or death).
A total of 11 478 patients were screened following ambulance transportation; 1391 were eligible and approached, but 177 did not consent. Of 1214 patients enrolled (mean [SD] age, 74.7 [13.2] years; 590 women [48.6%]), 500 were assessed by 242 paramedics trained in the PASTA intervention and 714 were assessed by 355 paramedics continuing with standard care. The paramedics trained in the PASTA intervention took a mean of 13.4 (95% CI, 9.4-17.4) minutes longer (P < .001) to complete patient care episodes. There was less thrombolysis among the patients in the PASTA group, but this was not significant (PASTA group, 197 of 500 patients [39.4%] vs the standard care group, 319 of 714 patients [44.7%]; adjusted odds ratio, 0.81 [95% CI, 0.61-1.08]; P = .15). Time from a paramedic on scene to thrombolysis was a mean of 8.5 minutes longer in the PASTA group (98.1 [37.6] minutes) vs the standard care group (89.4 [31.1] minutes; P = .01). Poor health outcomes did not differ significantly but occurred less often among patients in the PASTA group (313 of 489 patients [64.0%]) vs the standard care group (461 of 690 patients [66.8%]; adjusted odds ratio, 0.86 [95% CI, 0.60-1.20]; P = .39).
An enhanced paramedic assessment did not facilitate thrombolysis delivery. The unexpected combination of thrombolysis and health outcomes suggests possible alternative influences on treatment decisions by the intervention, requiring further evaluation.
ISRCTN Registry Identifier: ISRCTN12418919.
对于经过精心挑选的急性缺血性脑卒中患者,快速溶栓治疗可降低残疾程度,但服务提供具有挑战性。
确定增强型护理人员急性脑卒中治疗评估(PASTA)干预是否增加了医院溶栓率。
设计、设置和参与者:这是一项多中心、集群随机临床试验,于 2015 年 12 月至 2018 年 7 月在 3 个救护服务机构和 15 家医院进行。集群是基于救护站的护理人员,他们在随机分组前接受了 PASTA 或标准护理。如果医院专家确认了中风,并且护理人员在发病后 4 小时内开始评估,那么接受研究护理人员治疗的患者在入院后将被纳入研究。PASTA 或标准护理的分配反映了值班护理人员的随机分组状态。
PASTA 干预措施包括额外的院前信息收集、结构化的医院交接、交接后最多 15 分钟的实际协助、出发前护理检查表和临床医生反馈。标准护理反映了国家指南。
主要结局是接受溶栓治疗的患者比例。次要结局包括时间间隔和第 90 天的健康状况(不良状况定义为改良 Rankin 评分>2,表示依赖或死亡)。
在救护车转运后共筛选出 11478 名患者;有 1391 名符合条件并被邀请,但有 177 名不同意。在纳入的 1214 名患者中(平均[SD]年龄为 74.7[13.2]岁;590 名女性[48.6%]),500 名患者由接受过 PASTA 干预培训的 242 名护理人员进行评估,714 名患者由继续接受标准护理的 355 名护理人员进行评估。接受 PASTA 干预培训的护理人员完成患者护理的时间平均延长了 13.4 分钟(95%CI,9.4-17.4;P<0.001)。PASTA 组的溶栓患者较少,但无统计学意义(PASTA 组 500 名患者中有 197 名[39.4%],标准护理组 714 名患者中有 319 名[44.7%];调整后的优势比为 0.81[95%CI,0.61-1.08];P=0.15)。PASTA 组从护理人员到达现场到溶栓的时间平均延长了 8.5 分钟(98.1[37.6]分钟),而标准护理组为 89.4[31.1]分钟(P=0.01)。健康状况不佳的结局没有显著差异,但 PASTA 组(489 名患者中有 313 名[64.0%])发生的频率低于标准护理组(690 名患者中有 461 名[66.8%];调整后的优势比为 0.86[95%CI,0.60-1.20];P=0.39)。
增强型护理人员评估并未促进溶栓治疗的实施。溶栓治疗和健康结局的意外组合表明,干预措施可能对治疗决策产生其他影响,需要进一步评估。
ISRCTN 登记号:ISRCTN81011314。