Libby Peter
Division of Cardiovascular Medicine, Brigham and Women's Hospital and Harvard Medical School, Boston, Massachusetts.
JACC Basic Transl Sci. 2020 Apr 10;5(5):537-542. doi: 10.1016/j.jacbts.2020.04.001. eCollection 2020 May.
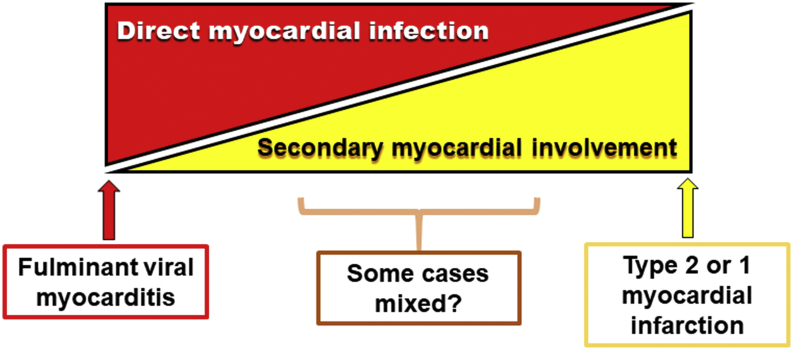
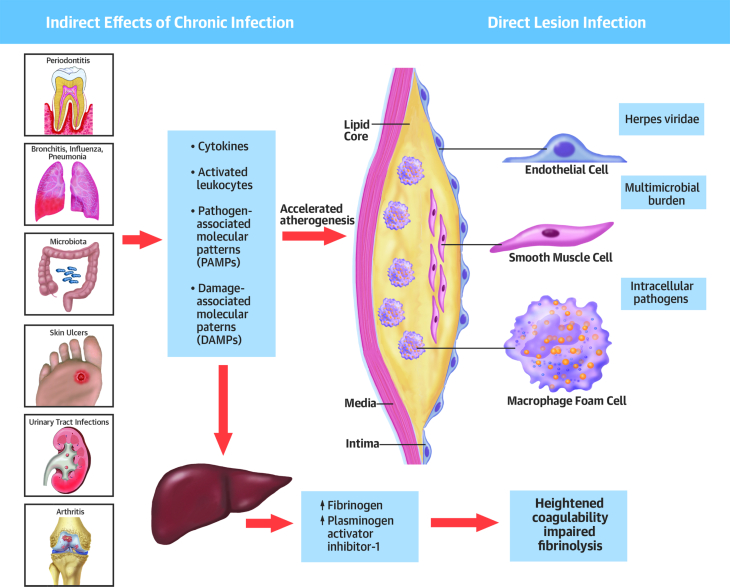
In the throes of the current coronavirus disease-2019 (COVID-19) pandemic, interest has burgeoned in the cardiovascular complications of this virulent viral infection. As troponin, a biomarker of cardiac injury, often rises in hospitalized patients, its interpretation and actionability require careful consideration. Fulminant myocarditis due to direct viral infection can certainly occur, but in patients with increased oxygen demands due to tachycardia and fever and reduced oxygen delivery due to hypotension and hypoxemia, COVID-19 disease can cause myocardial injury indirectly. Cytokines released during the acute infection can elicit activation of cells within pre-existing atherosclerotic lesions, augmenting thrombotic risk and risk of ischemic syndromes. Moreover, microvascular activation by cytokines can cause not only myocardial injury but can also harm other organ systems commonly involved in COVID-19 infections including the kidneys. Dealing with the immense challenge of COVID-19, confronted with severely ill patients in dire straits with virtually no rigorous evidence base to guide our therapy, we must call on our clinical skills and judgment. These touchstones can help guide us in selecting patients who might benefit from the advanced imaging and invasive procedures that present enormous logistical challenges in the current context. Lacking a robust evidence base, pathophysiologic reasoning can help guide our choices of therapy for individual clinical scenarios. We must exercise caution and extreme humility, as often plausible interventions fail when tested rigorously. But act today we must, and understanding the multiplicity of mechanisms of myocardial injury in COVID-19 infection will help us meet our mission unsupported by the comfort of strong data.
在当前2019冠状病毒病(COVID-19)大流行的阵痛中,人们对这种烈性病毒感染的心血管并发症的兴趣迅速增长。由于肌钙蛋白作为心脏损伤的生物标志物,在住院患者中常常升高,因此对其解读和可操作性需要仔细考虑。直接病毒感染导致的暴发性心肌炎肯定会发生,但在因心动过速和发热导致氧需求增加以及因低血压和低氧血症导致氧输送减少的患者中,COVID-19疾病可间接导致心肌损伤。急性感染期间释放的细胞因子可引发已存在的动脉粥样硬化病变内细胞的激活,增加血栓形成风险和缺血综合征风险。此外,细胞因子引起的微血管激活不仅可导致心肌损伤,还可损害COVID-19感染中常见的其他器官系统,包括肾脏。应对COVID-19这一巨大挑战,面对病情严重、处境危急且几乎没有严格证据基础来指导我们治疗的患者,我们必须依靠我们的临床技能和判断力。这些试金石可帮助我们选择可能从先进影像学检查和侵入性操作中获益的患者,而在当前情况下这些操作带来了巨大的后勤挑战。由于缺乏强有力的证据基础,病理生理推理可帮助指导我们针对个体临床情况选择治疗方法。我们必须谨慎行事并保持极度谦逊,因为通常看似合理的干预措施在经过严格测试时往往会失败。但我们今天必须采取行动,了解COVID-19感染中心肌损伤的多种机制将有助于我们在缺乏有力数据支持的情况下完成我们的使命。