Center of Emergency Medicine, University Hospital Essen, Hufelandstrasse 55, 45122, Essen, Germany.
Department of Anesthesiology and Intensive Care Medicine, Philipps-University Marburg, 35033, Marburg, Germany.
BMC Emerg Med. 2020 Mar 23;20(1):22. doi: 10.1186/s12873-020-00316-z.
Videolaryngoscopy (VL) has become a popular method of intubation (ETI). Although VL may facilitate ETI in less-experienced rescuers there are limited data available concerning ETI performed by paramedics during CPR. The goal was to evaluate the impact VL compared with DL on intubation success and glottic view during CPR performed by German paramedics. We investigated in an observational prospective study the superiority of VL by paramedics during CPR compared with direct laryngoscopy (DL).
In a single Emergency Medical Service (EMS) in Germany with in total 32 ambulances paramedics underwent an initial instruction from in endotracheal intubation (ETI) with GlideScope® (GVL) during resuscitation. The primary endpoint was good visibility of the glottis (Cormack-Lehane grading 1/2), and the secondary endpoint was successful intubation comparing GVL and DL.
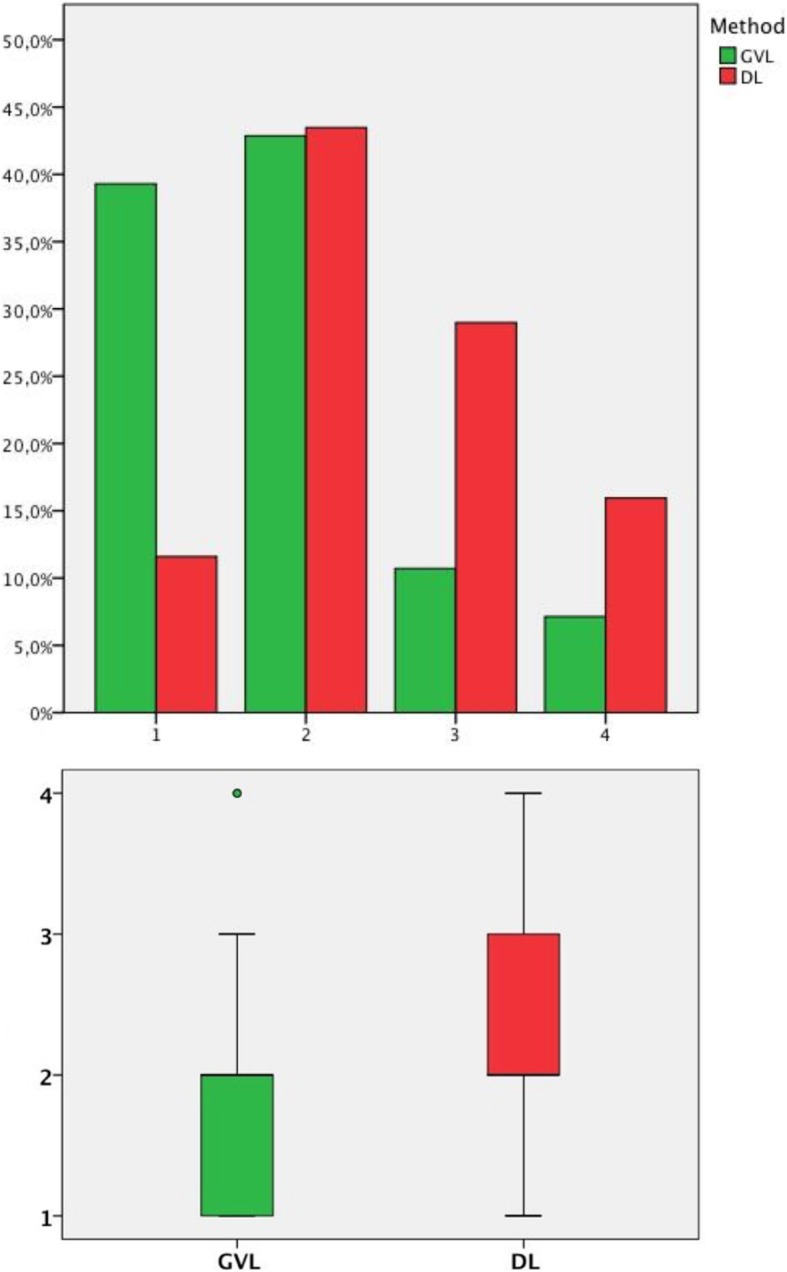
In total n = 97 patients were included, n = 69 with DL (n = 85 intubation attempts) and n = 28 VL (n = 37 intubation attempts). Videolaryngoscopy resulted in a significantly improved visualization of the larynx compared with DL. In the group using GVL, 82% rated visualization of the glottis as CL 1&2 versus 55% in the DL group (p = 0.02). Despite better visualization of the larynx, there was no statistically significant difference in successful ETI between GVL and DL (GVL 75% vs. DL 68.1%, p = 0.63).
We found no difference in Overall and First Pass Success (FPS) between GVL and DL during CPR by German paramedics despite better glottic visualization with GVL. Therefore, we conclude that education in VL should also focus on insertion of the endotracheal tube, considering the different procedures of GVL.
German Clinical Trial Register DRKS00020976, 27. February 2020 retrospectively registered.
视频喉镜(VL)已成为一种流行的插管方法(ETI)。尽管 VL 可能使经验较少的救援人员更容易进行 ETI,但关于在 CPR 期间由护理人员进行的 ETI 可用数据有限。目的是评估 VL 与 DL 相比对德国护理人员进行 CPR 时插管成功率和声门视图的影响。我们在一项观察性前瞻性研究中调查了在 CPR 期间 VL 相对于直接喉镜(DL)的优越性。
在德国的一个单一的紧急医疗服务(EMS)中,共有 32 辆救护车,护理人员在复苏期间接受了 GlideScope®(GVL)的初始气管内插管(ETI)指导。主要终点是声门的良好可视性(Cormack-Lehane 分级 1/2),次要终点是比较 GVL 和 DL 的成功插管。
共有 97 例患者纳入研究,69 例使用 DL(85 次插管尝试)和 28 例 VL(37 次插管尝试)。与 DL 相比,视频喉镜可显著改善喉镜的可视化效果。在使用 GVL 的组中,82%的人将声门的可视化评为 CL 1&2,而 DL 组为 55%(p=0.02)。尽管喉部的可视化效果更好,但 GVL 和 DL 之间在 ETI 的成功率方面没有统计学上的显著差异(GVL 为 75%,DL 为 68.1%,p=0.63)。
尽管 GVL 可更好地可视化声门,但我们发现德国护理人员在 CPR 期间,使用 GVL 和 DL 进行 ETI 时,在整体和首次通过成功率(FPS)方面没有差异。因此,我们得出结论,VL 的教育也应侧重于气管内导管的插入,同时考虑到 GVL 的不同程序。
德国临床试验注册处 DRKS00020976,2020 年 2 月 27 日回顾性注册。