Infection, Inflammation and Rheumatology Section, UCL Great Ormond Street Institute for Child Health, London, UK.
Rheumatology Section, Great Ormond Street Hospital for Children NHS Trust, Level 6 Southwood Building, Great Ormond Street, London, WC1N 3JH, UK.
Arthritis Res Ther. 2020 Apr 15;22(1):79. doi: 10.1186/s13075-020-02164-5.
Anti-TNF treatment may be useful for the treatment of patients with refractory juvenile dermatomyositis (JDM). The aim of this study was to describe the use of infliximab and adalimumab therapy in juvenile dermatomyositis as an adjunctive treatment.
Sixty children recruited to the UK JDM Cohort and Biomarker Study that had received at least 3 months of anti-TNF treatment (infliximab or adalimumab) were studied. Childhood Myositis Assessment Scale (CMAS), Manual Muscle Testing (MMT8) and physician's global assessment (PGA) were recorded. Skin disease was assessed using the modified skin disease activity score (DAS). Data were analysed using Friedman's test for repeated measures analysis of variance.
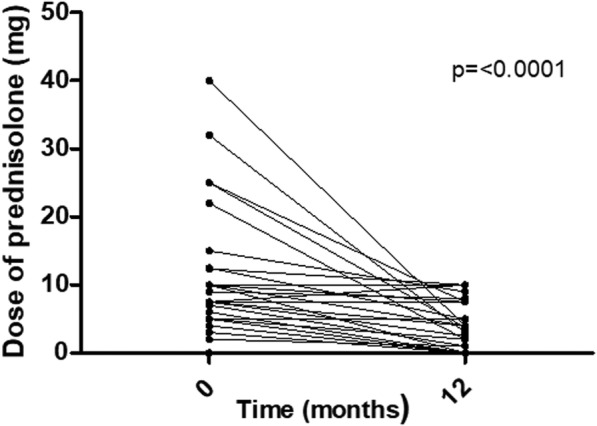
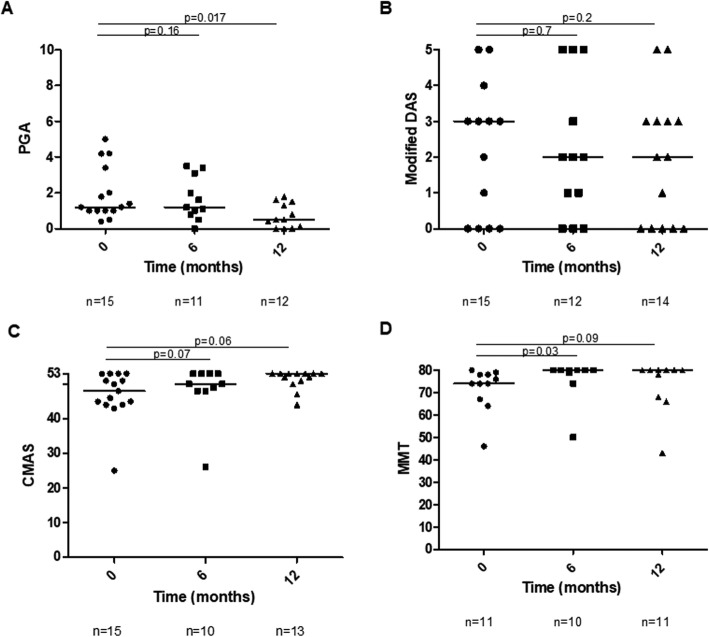
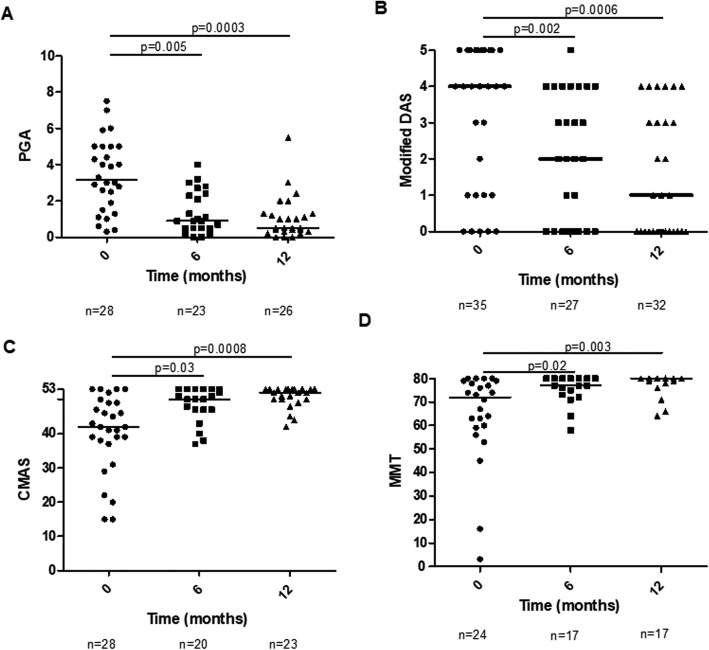
Compared to baseline, there were improvements at 6 and 12 months in skin disease (χ(2) = 15.52, p = 0.00043), global disease (χ(2) = 8.14, p = 0.017) and muscle disease (CMAS χ(2) = 17.02, p = 0.0002 and MMT χ(2) = 10.56, p = 0.005) in infliximab patients. For patients who switched from infliximab to adalimumab, there was improvement in global disease activity (χ(2) = 6.73, p = 0.03), and trends towards improvement in CMAS, MMT8 and modified DAS. The median initial prednisolone dose was 6 [0-10] mg, and final was 2.5 [0-7.5] mg (p < 0.0001). Fifty-four per cent of patients had a reduction in the number and/or size of calcinosis lesions. Twenty-five per cent switched their anti-TNF treatment from infliximab to adalimumab. 66.7%of the switches were to improve disease control, 26.7% due to adverse events and 6.6% due to patient preference. A total of 13.9 adverse reactions occurred in 100 patient-years, of which 5.7 were considered serious.
Reductions in muscle and skin disease, including calcinosis, were seen following treatment with infliximab and adalimumab.
抗 TNF 治疗可能对治疗难治性幼年特发性皮肌炎(JDM)患者有用。本研究旨在描述英夫利昔单抗和阿达木单抗作为辅助治疗在幼年皮肌炎中的应用。
对英国 JDM 队列和生物标志物研究中至少接受 3 个月抗 TNF 治疗(英夫利昔单抗或阿达木单抗)的 60 名儿童进行研究。记录儿童肌炎评估量表(CMAS)、手动肌肉测试(MMT8)和医生整体评估(PGA)。皮肤疾病采用改良皮肤疾病活动评分(DAS)进行评估。使用 Friedman 重复测量方差分析检验对数据进行分析。
与基线相比,英夫利昔单抗治疗的患儿在 6 个月和 12 个月时皮肤疾病(χ(2) = 15.52,p = 0.00043)、整体疾病(χ(2) = 8.14,p = 0.017)和肌肉疾病(CMAS χ(2) = 17.02,p = 0.0002 和 MMT χ(2) = 10.56,p = 0.005)均有改善。对于从英夫利昔单抗转为阿达木单抗的患者,整体疾病活动度有所改善(χ(2) = 6.73,p = 0.03),CMAS、MMT8 和改良 DAS 也有改善的趋势。初始泼尼松龙剂量中位数为 6 [0-10]mg,最终为 2.5 [0-7.5]mg(p<0.0001)。54%的患者钙沉积病变的数量和/或大小减少。25%的患者将抗 TNF 治疗从英夫利昔单抗转为阿达木单抗。66.7%的转换是为了改善疾病控制,26.7%是因为不良反应,6.6%是因为患者偏好。在 100 患者年中发生了 13.9 次不良反应,其中 5.7 次被认为是严重的。
英夫利昔单抗和阿达木单抗治疗后肌肉和皮肤疾病(包括钙沉积)均有改善。