AlSharoqi Isa Ahmed, Aljumah Mohamed, Bohlega Saeed, Boz Cavit, Daif Abdelkader, El-Koussa Salam, Inshasi Jihad, Kurtuncu Murat, Müller Thomas, Retief Chris, Sahraian Mohammad Ali, Shaygannejad Vahid, Slassi Ilham, Taha Karim, Zakaria Magd, Sørensen Per Soelberg
Department of Clinical Neurosciences, Salmaniya Medical Complex, PO Box 12, Manama, Bahrain.
King Fahad Medical City, Ministry of Health, Riyadh, Kingdom of Saudi Arabia.
Neurol Ther. 2020 Jun;9(1):55-66. doi: 10.1007/s40120-020-00187-3. Epub 2020 Apr 15.
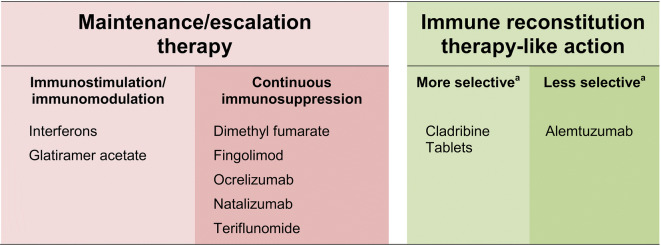
The majority of disease-modifying drugs (DMDs) available for the management of active relapsing-remitting multiple sclerosis (RMS) depend on continuous drug intake for maintained efficacy, with escalation to a more active drug when an unacceptable level of disease activity returns. Among continuously applied regimens, interferons and glatiramer acetate act as immunomodulators, while dimethyl fumarate, fingolimod, ocrelizumab, natalizumab and teriflunomide are associated with continuous immunosuppression. By contrast, immune reconstitution therapy (IRT) provides efficacy that outlasts a short course of treatment. Autologous hemopoietic stem cell transplantation is perhaps the classic example of IRT, but this invasive and intensive therapy has challenging side-effects. A short treatment course of a pharmacologic agent hypothesized to act as an IRT, such as Cladribine Tablets 3.5 mg/kg or alemtuzumab, can provide long-term suppression of MS disease activity, without need for continuous treatment (the anti-CD20 mechanism of ocrelizumab has the potential to act as an IRT, but is administered continuously, at 6-monthly intervals). Cladribine Tablets 3.5 mg/kg shows some selectivity in targeting adaptive immunity with a lesser effect on innate immunity. The introduction of IRT-like disease-modifying drugs (DMDs) challenges the traditional maintenance/escalation mode of treatment and raises new questions about how disease activity is measured. In this review, we consider a modern classification of DMDs for MS and its implications for the care of patients in the IRT era.
大多数可用于治疗复发缓解型多发性硬化症(RMS)活动期的疾病修正药物(DMDs)都依赖持续用药以维持疗效,当疾病活动水平达到不可接受的程度时则升级使用更有效的药物。在持续应用的治疗方案中,干扰素和醋酸格拉替雷作为免疫调节剂发挥作用,而富马酸二甲酯、芬戈莫德、奥瑞珠单抗、那他珠单抗和特立氟胺则与持续免疫抑制相关。相比之下,免疫重建疗法(IRT)提供的疗效在短疗程治疗后仍能持续。自体造血干细胞移植可能是IRT的经典例子,但这种侵入性强且强度大的治疗有具有挑战性的副作用。一种被假设为IRT的药物(如3.5mg/kg的克拉屈滨片或阿仑单抗)的短疗程治疗可以长期抑制MS疾病活动,而无需持续治疗(奥瑞珠单抗的抗CD20机制有可能作为一种IRT,但需每6个月持续给药)。3.5mg/kg的克拉屈滨片在靶向适应性免疫方面表现出一定的选择性,对固有免疫的影响较小。类似IRT的疾病修正药物(DMDs)的引入挑战了传统的维持/升级治疗模式,并对如何测量疾病活动提出了新问题。在本综述中,我们考虑了MS的DMDs现代分类及其在IRT时代对患者护理的影响。