Division of Nephrology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan, Republic of China.
Division of Cardiology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan, Republic of China.
Stem Cells Transl Med. 2020 Aug;9(8):827-838. doi: 10.1002/sctm.19-0409. Epub 2020 Apr 16.
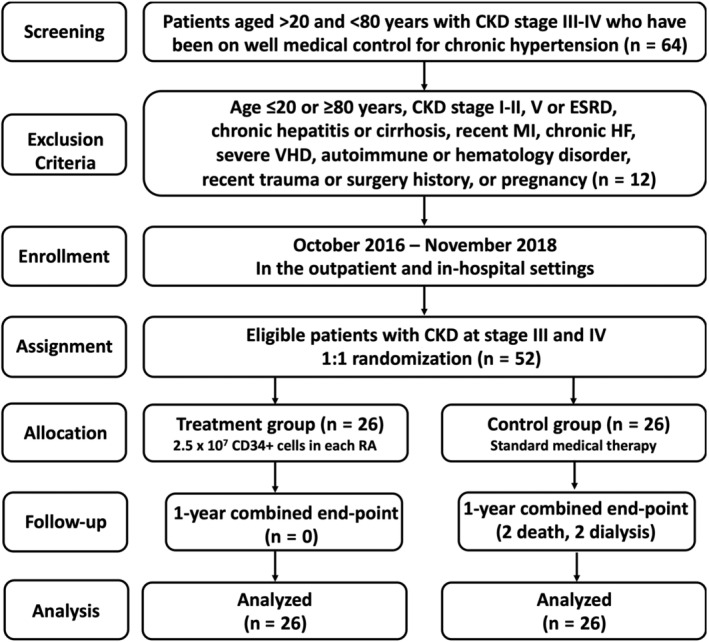
This was a randomized, open-label, controlled phase II clinical trial to investigate the safety, efficacy, and outcomes of intrarenal artery infusion of autologous peripheral-blood-derived CD34+ cells for patients with chronic kidney disease (CKD; ie, stage III or IV).
Between October 2016 and July 2018, 52 consecutive patients with CKD at stage III or IV were randomly allocated into a treatment group (TG; 2.5 × 10 cells for each intrarenal artery; n = 26) and a control group (CG; standardized pharmacotherapy only; n = 26). The primary endpoints included safety and change of creatinine level/creatinine clearance. The secondary endpoints were 12-month combined unfavorable clinical outcomes (defined as dialysis or death), improvement in proteinuria, and CD34+ cell-related adverse events.
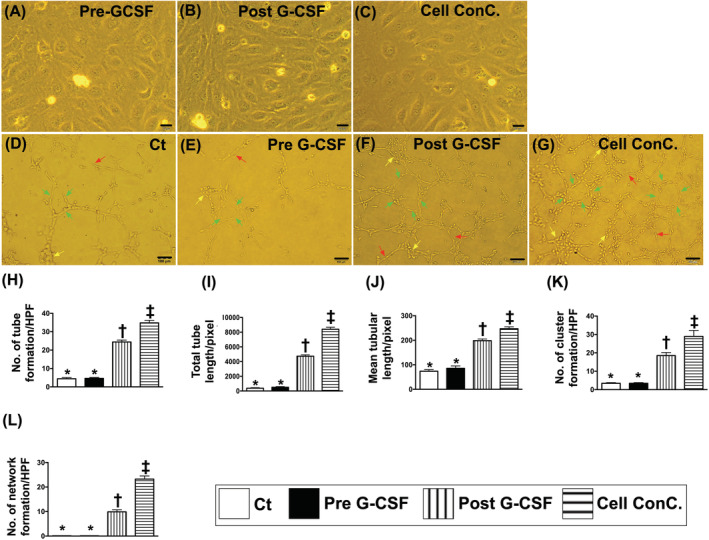
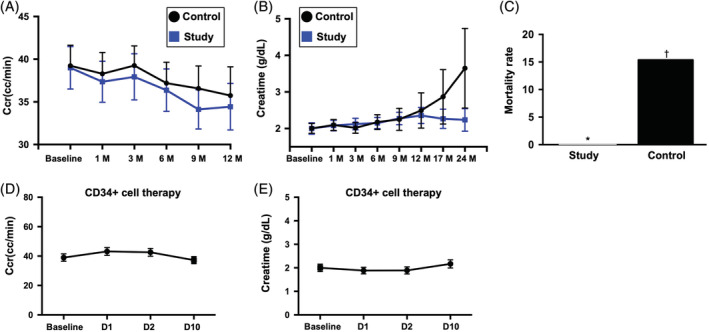
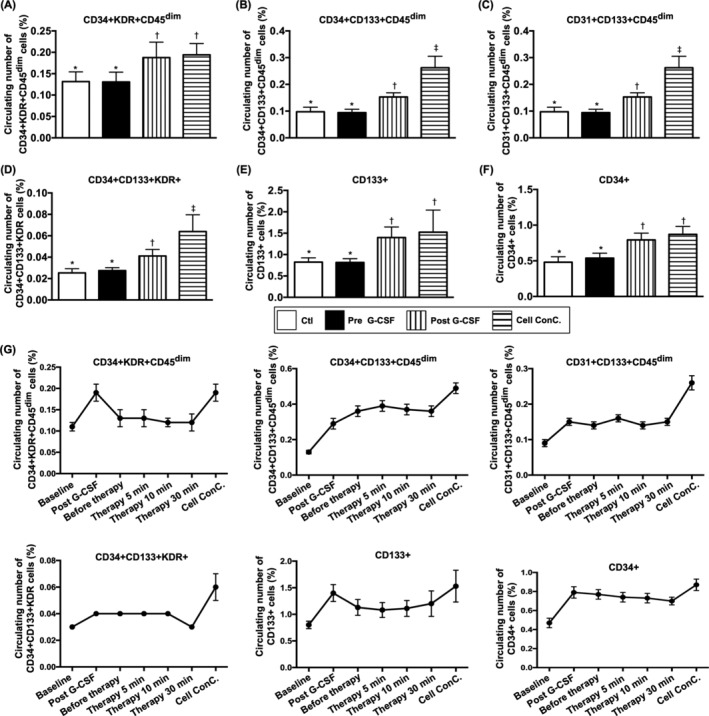
All patients were uneventfully discharged after CD34+ cell therapy. The baseline endothelial progenitor cell (EPC) populations did not differ between TG and CG (P > .5). Flow cytometric analysis showed increases in circulating EPC (ie, CD34+KDR+CD45 / CD34+CD133+CD45 /CD31+CD133+CD45 /CD34+CD133+KDR+/CD133+) and hematopoietic stem cell (CD34+) populations after granulocyte-colony stimulating factor treatment (all P < .001). Besides, Matrigel assay of angiogenesis was also significantly enhanced (all P < .001). Renal-venous blood samplings (ie, at 0, 5, 10, and 30 minutes after CD34+ cell infusion) demonstrated significant progressive increases in EPC level (P for trend <.001) among the TG patients. One-year combined unfavorable clinical outcomes were significantly lower in TG than those in CG (0% [0] vs 13.3% [4], P = .038). By 12 months after CD34+ cell therapy, circulating creatinine level, ratio of urine protein to urine creatinine, and creatinine clearance showed no difference between TG and CG (all P > .1).
CD34+ cell therapy was safe and improved 1-year outcome.
这是一项随机、开放标签、对照的 II 期临床试验,旨在研究经肾内动脉输注自体外周血源性 CD34+细胞治疗慢性肾脏病(CKD;即 III 或 IV 期)患者的安全性、疗效和结局。
2016 年 10 月至 2018 年 7 月,连续纳入 52 例 CKD III 或 IV 期患者,随机分为治疗组(每组肾内动脉内输注 2.5×10 个细胞;n=26)和对照组(仅接受标准化药物治疗;n=26)。主要终点包括安全性和肌酐水平/肌酐清除率的变化。次要终点为 12 个月时联合不良临床结局(定义为透析或死亡)、蛋白尿改善以及与 CD34+细胞相关的不良事件。
所有患者在接受 CD34+细胞治疗后均顺利出院。治疗组和对照组的基线内皮祖细胞(EPC)群体无差异(P>.5)。流式细胞术分析显示,粒细胞集落刺激因子治疗后循环 EPC(即 CD34+KDR+CD45/CD34+CD133+CD45/CD31+CD133+CD45/CD34+CD133+KDR+/CD133+)和造血干细胞(CD34+)群体增加(均 P<.001)。此外,血管生成的 Matrigel 检测也显著增强(均 P<.001)。肾静脉血取样(即 CD34+细胞输注后 0、5、10 和 30 分钟)显示治疗组 EPC 水平呈显著渐进性增加(趋势 P<.001)。治疗组 1 年联合不良临床结局明显低于对照组(0%[0] vs 13.3%[4],P=.038)。CD34+细胞治疗后 12 个月,治疗组和对照组的循环肌酐水平、尿蛋白与尿肌酐比值以及肌酐清除率无差异(均 P>.1)。
CD34+细胞治疗安全,可改善 1 年结局。