Department of Cardiology, Leiden University Medical Center, Leiden, the Netherlands.
JAMA Netw Open. 2020 Apr 1;3(4):e202165. doi: 10.1001/jamanetworkopen.2020.2165.
Smart technology via smartphone-compatible devices might improve blood pressure (BP) regulation in patients after myocardial infarction.
To investigate whether smart technology in clinical practice can improve BP regulation and to evaluate the feasibility of such an intervention.
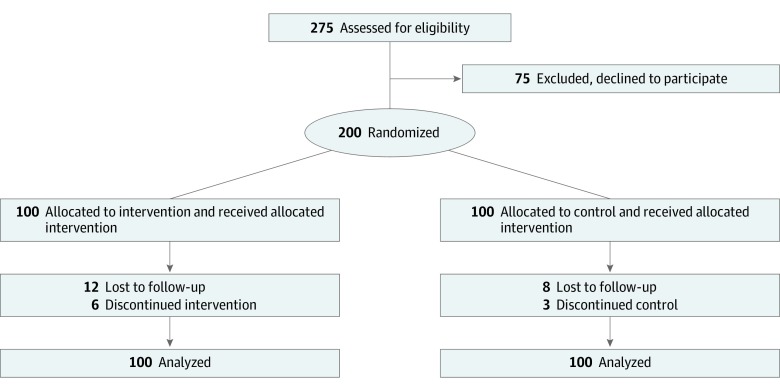
DESIGN, SETTING, AND PARTICIPANTS: This study was an investigator-initiated, single-center, nonblinded, feasibility, randomized clinical trial conducted at the Department of Cardiology of the Leiden University Medical Center between May 2016 and December 2018. Two hundred patients, who were admitted with either ST-segment elevation myocardial infarction or non-ST-segment acute coronary syndrome, were randomized in a 1:1 fashion between follow-up groups using smart technology and regular care. Statistical analysis was performed from January 2019 to March 2019.
For patients randomized to regular care, 4 physical outpatient clinic visits were scheduled in the year following the initial event. In the intervention group, patients were given 4 smartphone-compatible devices (weight scale, BP monitor, rhythm monitor, and step counter). In addition, 2 in-person outpatient clinic visits were replaced by electronic visits.
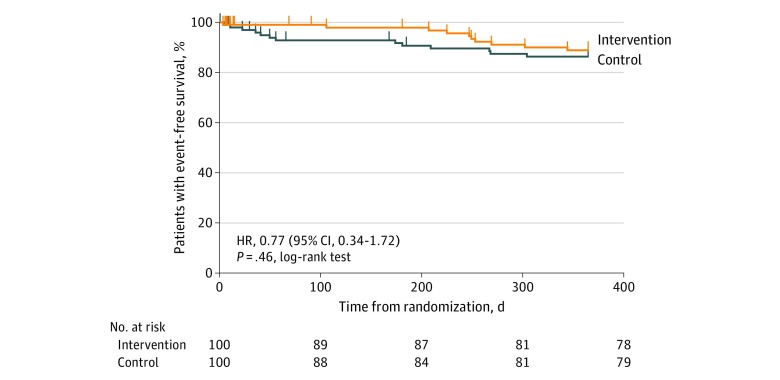
The primary outcome was BP control. Secondary outcomes, as a parameter of feasibility, included patient satisfaction (general questionnaire and smart technology-specific questionnaire), measurement adherence, all-cause mortality, and hospitalizations for nonfatal adverse cardiac events.
In total, 200 patients (median age, 59.7 years [interquartile range, 52.9-65.6 years]; 156 men [78%]) were included, of whom 100 were randomized to the intervention group and 100 to the control group. After 1 year, 79% of patients in the intervention group had controlled BP vs 76% of patients in the control group (P = .64). General satisfaction with care was the same between groups (mean [SD] scores, 82.6 [14.1] vs 82.0 [15.1]; P = .88). The all-cause mortality rate was 2% in both groups (P > .99). A total of 20 hospitalizations for nonfatal adverse cardiac events occurred (8 in the intervention group and 12 in the control group). Of all patients, 32% sent in measurements each week, with 63% sending data for more than 80% of the weeks they participated in the trial. In the intervention group only, 90.3% of patients were satisfied with the smart technology intervention.
These findings suggest that smart technology yields similar percentages of patients with regulated BP compared with the standard of care. Such an intervention is feasible in clinical practice and is accepted by patients. More research is mandatory to improve patient selection of such an intervention.
ClinicalTrials.gov Identifier: NCT02976376.
通过智能手机兼容设备实现的智能技术可能改善心肌梗死后患者的血压(BP)调节。
研究智能技术在临床实践中是否可以改善 BP 调节,并评估这种干预的可行性。
设计、地点和参与者:这是一项由研究人员发起的、单中心、非盲、可行性、随机临床试验,在 2016 年 5 月至 2018 年 12 月期间在莱顿大学医学中心的心脏病科进行。200 名患者因 ST 段抬高型心肌梗死或非 ST 段急性冠脉综合征入院,采用智能技术和常规护理的方式以 1:1 的比例随机分配到随访组。统计分析于 2019 年 1 月至 2019 年 3 月进行。
对于随机分配到常规护理的患者,在初始事件发生后的一年中安排了 4 次门诊随访。在干预组中,患者被提供了 4 个智能手机兼容设备(体重秤、血压监测器、心律监测器和计步器)。此外,通过电子就诊代替了 2 次门诊就诊。
主要结局是 BP 控制。次要结局(作为可行性的参数)包括患者满意度(一般问卷和智能技术特定问卷)、测量依从性、全因死亡率和非致命性不良心脏事件住院率。
共纳入 200 名患者(中位数年龄 59.7 岁[四分位间距,52.9-65.6 岁];156 名男性[78%]),其中 100 名被随机分配到干预组,100 名被分配到对照组。1 年后,干预组中 79%的患者血压得到控制,而对照组中 76%的患者血压得到控制(P = .64)。两组患者对护理的总体满意度相同(平均[标准差]评分,82.6 [14.1]与 82.0 [15.1];P = .88)。两组的全因死亡率均为 2%(P > .99)。共发生 20 例非致命性不良心脏事件住院(干预组 8 例,对照组 12 例)。所有患者中,每周有 32%的人发送测量值,其中 63%的人发送数据的周数超过他们参与试验的 80%。仅在干预组中,90.3%的患者对智能技术干预表示满意。
这些发现表明,与标准护理相比,智能技术使具有调节 BP 的患者百分比相似。这种干预在临床实践中是可行的,并且被患者接受。需要进一步的研究来改善这种干预的患者选择。
ClinicalTrials.gov 标识符:NCT02976376。