Department of Public Health and Primary Care, University of Cambridge, Cambridge, UK.
Department of Urology, Cambridge University Hospitals Trust, Cambridge, UK.
BMC Med. 2020 Apr 17;18(1):95. doi: 10.1186/s12916-020-01548-3.
The clinical pathway to detect and diagnose prostate cancer has been revolutionised by the use of multiparametric MRI (mpMRI pre-biopsy). mpMRI however remains a resource-intensive test and is highly operator dependent with variable effectiveness with regard to its negative predictive value. Here we tested the use of the phi assay in standard clinical practice to pre-select men at the highest risk of harbouring significant cancer and hence refine the use of mpMRI and biopsies.
A prospective five-centre study recruited men being investigated through an mpMRI-based prostate cancer diagnostic pathway. Test statistics for PSA, PSA density (PSAd) and phi were assessed for detecting significant cancers using 2 definitions: ≥ Grade Group (GG2) and ≥ Cambridge Prognostic Groups (CPG) 3. Cost modelling and decision curve analysis (DCA) was simultaneously performed.
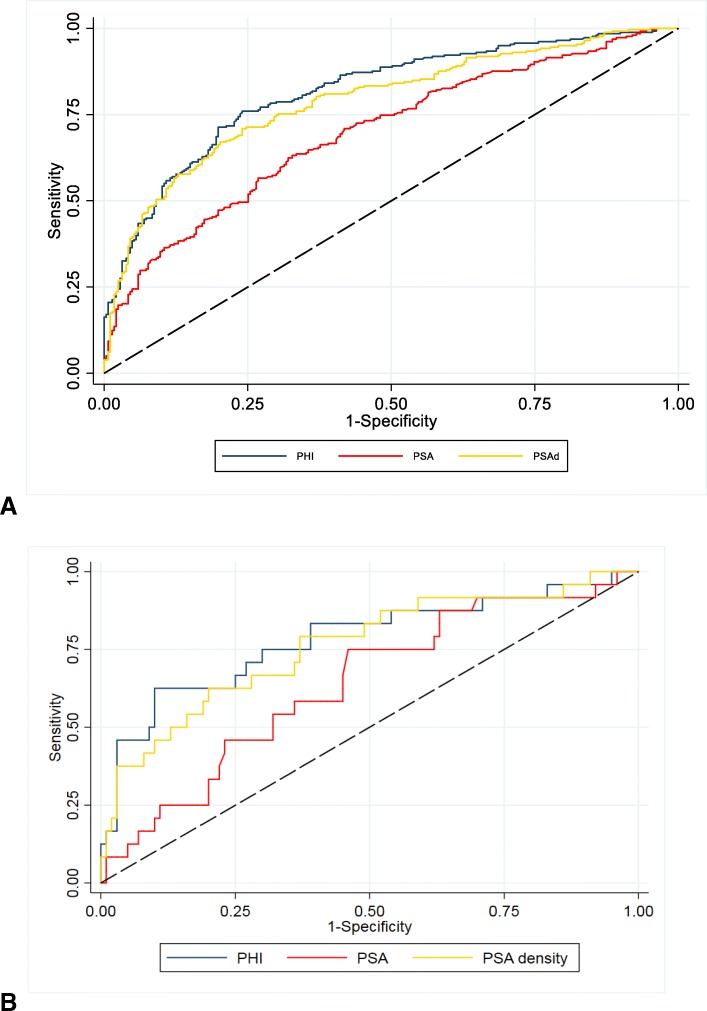
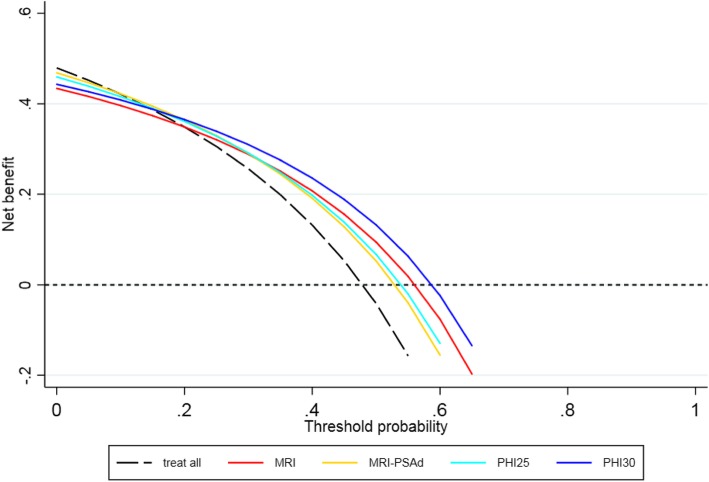
A total of 545 men were recruited and studied with a median age, PSA and phi of 66 years, 8.0 ng/ml and 44 respectively. Overall, ≥ GG2 and ≥ CPG3 cancer detection rates were 64% (349/545), 47% (256/545) and 32% (174/545) respectively. There was no difference across centres for patient demographics or cancer detection rates. The overall area under the curve (AUC) for predicting ≥ GG2 cancers was 0.70 for PSA and 0.82 for phi. AUCs for ≥ CPG3 cancers were 0.81 and 0.87 for PSA and phi respectively. AUC values for phi did not differ between centres suggesting reliability of the test in different diagnostic settings. Pre-referral phi cut-offs between 20 and 30 had NPVs of 0.85-0.90 for ≥ GG2 cancers and 0.94-1.0 for ≥ CPG3 cancers. A strategy of mpMRI in all and biopsy only positive lesions reduced unnecessary biopsies by 35% but missed 9% of ≥ GG2 and 5% of ≥ CPG3 cancers. Using PH ≥ 30 to rule out referrals missed 8% and 5% of ≥ GG2 and ≥ CPG3 cancers (and reduced unnecessary biopsies by 40%). This was achieved however with 25% fewer mpMRI. Pathways incorporating PSAd missed fewer cancers but necessitated more unnecessary biopsies. The phi strategy had the lowest mean costs with DCA demonstrating net clinical benefit over a range of thresholds.
phi as a triaging test may be an effective way to reduce mpMRI and biopsies without compromising detection of significant prostate cancers.
多参数 MRI(mpMRI 活检前)的使用彻底改变了前列腺癌的检测和诊断临床路径。然而,mpMRI 仍然是一种资源密集型检测方法,并且高度依赖操作人员,其阴性预测值的效果存在差异。在这里,我们在标准临床实践中测试了 phi 分析的使用,以预先选择患高风险显著癌症的男性,从而精减 mpMRI 和活检的应用。
一项前瞻性的五中心研究招募了通过基于 mpMRI 的前列腺癌诊断途径进行检查的男性。使用两种定义(≥分级组(GG2)和≥剑桥预后组(CPG)3)评估 PSA、PSA 密度(PSAd)和 phi 的检测统计数据,以检测显著癌症。同时进行成本建模和决策曲线分析(DCA)。
共招募了 545 名男性进行研究,中位年龄、PSA 和 phi 分别为 66 岁、8.0ng/ml 和 44。总体而言,≥ GG2 和≥ CPG3 癌症的检出率分别为 64%(349/545)、47%(256/545)和 32%(174/545)。不同中心的患者人口统计学特征或癌症检出率无差异。预测≥ GG2 癌症的总体曲线下面积(AUC)为 PSA 的 0.70 和 phi 的 0.82。预测≥ CPG3 癌症的 AUC 分别为 PSA 和 phi 的 0.81 和 0.87。phi 的 AUC 值在不同中心之间没有差异,表明该检测在不同诊断环境中的可靠性。phi 的预转诊截断值在 20 到 30 之间时,≥ GG2 癌症的阴性预测值为 0.85-0.90,≥ CPG3 癌症的阴性预测值为 0.94-1.0。所有患者进行 mpMRI 检查和仅对阳性病变进行活检的策略减少了 35%的不必要活检,但漏诊了 9%的≥ GG2 和 5%的≥ CPG3 癌症。使用 PH≥30 排除转诊患者漏诊了 8%和 5%的≥ GG2 和≥ CPG3 癌症(并减少了 40%的不必要活检)。然而,这一策略减少了 25%的 mpMRI。纳入 PSAd 的策略漏诊的癌症较少,但需要更多不必要的活检。DCA 表明,在一系列阈值下,phi 策略的平均成本最低,具有净临床获益。
phi 作为一种分诊检测方法,可能是一种在不影响显著前列腺癌检出率的情况下减少 mpMRI 和活检的有效方法。