Department of Gynecology and Obstetrics, Copenhagen University Hospital Holbæk, Holbæk, Denmark.
Department of Clinical Biochemistry, Herlev and Gentofte Hospital, Hellerup, Denmark.
PLoS One. 2020 Apr 17;15(4):e0231657. doi: 10.1371/journal.pone.0231657. eCollection 2020.
Low levels of vitamin D in pregnancy have been associated with the risk of a variety of pregnancy outcomes. Few studies have investigated vitamin D concentrations throughout pregnancy in healthy women, and most guidelines recommend high vitamin D levels. In the present study, we investigated 25-hydroxyvitamin D concentrations in healthy Caucasian Danish women in relation to season, gestational age and possible vitamin D-linked complications.
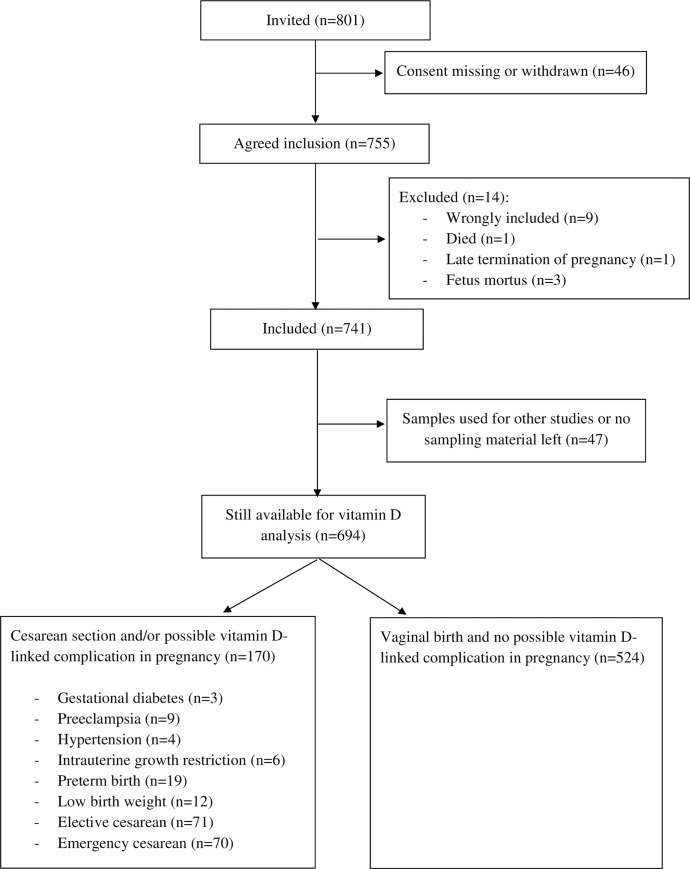
Eight hundred and one healthy Caucasian Danish women with an expected normal pregnancy were recruited among 2147 women attending first trimester screening. Seven blood samplings were planned throughout the pregnancy and delivery period. The 25-hydroxyvitamin D2 (25(OH)D2) and 25-hydroxyvitamin D3 (25(OH)D3) concentrations were measured by LC-MS/MS and total 25-hydroxyvitamin D (25(OH)D) were calculated.
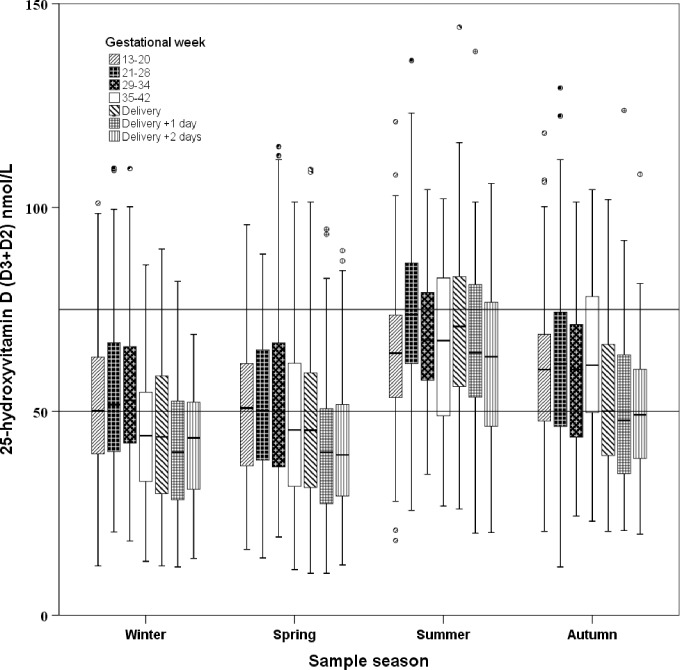
A total of 3304 samples from 694 women were available for 25(OH)D measurements. The mean (25th-75th percentiles) concentrations of 25(OH)D, 25(OH)D3, and 25(OH)D2 were 54.6 (38.8-68.6) nmol/L, 52.2 (36.4-66.4) nmol/L, and 2.4 (2.2-2.2) nmol/L, respectively. Season was the strongest predictor of 25(OH)D concentration, with the lowest values observed in winter and spring, where only 42% and 41% of samples, respectively, were above 50 nmol/L. Nearly all women had values below the suggested optimal level of 75 nmol/L, independent of season. 25(OH)D peaked at gestational weeks 21-34. Plasma 25(OH)D2 levels were low in all seasons. Women with complications during pregnancy had higher 25(OH)D (estimated difference 9.8 nmol/L, standard error 2.7, p<0.001) than did women without complications, and women giving birth vaginally had lower 25(OH)D than did those delivering via elective (10.0 nmol/L, standard error 2.1, p<0.001) or emergency cesarean section (6.8 nmol/L, standard error 2.2, p<0.001).
The 25(OH)D concentrations vary with both season and gestational age. Healthy women had lower 25(OH)D concentrations than recommended, without an association with an increased risk of pregnancy complications. Guidelines for vitamin D in pregnancy may require revision.
妊娠期间维生素 D 水平较低与各种妊娠结局的风险有关。很少有研究调查过健康女性在整个妊娠期间的维生素 D 浓度,大多数指南建议高维生素 D 水平。在本研究中,我们调查了 801 名健康的丹麦白种人女性,以了解维生素 D 与季节、孕龄和可能的维生素 D 相关并发症之间的关系。
在 2147 名接受早孕筛查的女性中,招募了 801 名预计正常妊娠的健康丹麦白种人女性。整个妊娠和分娩期间计划进行 7 次采血。通过 LC-MS/MS 测量 25-羟维生素 D2(25(OH)D2)和 25-羟维生素 D3(25(OH)D3)浓度,并计算总 25-羟维生素 D(25(OH)D)。
共有 694 名女性的 3304 个样本可用于 25(OH)D 测量。25(OH)D、25(OH)D3 和 25(OH)D2 的平均(25 百分位数-75 百分位数)浓度分别为 54.6(38.8-68.6)nmol/L、52.2(36.4-66.4)nmol/L 和 2.4(2.2-2.2)nmol/L。季节是 25(OH)D 浓度的最强预测因子,冬季和春季的浓度最低,分别只有 42%和 41%的样本浓度超过 50 nmol/L。几乎所有女性的维生素 D 水平都低于 75 nmol/L 的建议最佳水平,与季节无关。25(OH)D 在妊娠 21-34 周时达到峰值。所有季节的血浆 25(OH)D2 水平均较低。与无并发症的女性相比,妊娠期间有并发症的女性 25(OH)D 水平更高(估计差异 9.8 nmol/L,标准误差 2.7,p<0.001),与选择性(10.0 nmol/L,标准误差 2.1,p<0.001)或紧急剖宫产(6.8 nmol/L,标准误差 2.2,p<0.001)分娩的女性相比,阴道分娩的女性 25(OH)D 水平较低。
25(OH)D 浓度随季节和孕龄而变化。健康女性的 25(OH)D 浓度低于推荐水平,与妊娠并发症风险增加无关。妊娠维生素 D 指南可能需要修订。