Division of Cardiothoracic Anesthesiology, Department of Anesthesiology, Vanderbilt University Medical Center, Nashville, TN.
Division of Critical Care Medicine, Department of Anesthesiology, Vanderbilt University Medical Center, Nashville, TN.
Semin Nephrol. 2020 Mar;40(2):173-187. doi: 10.1016/j.semnephrol.2020.01.008.
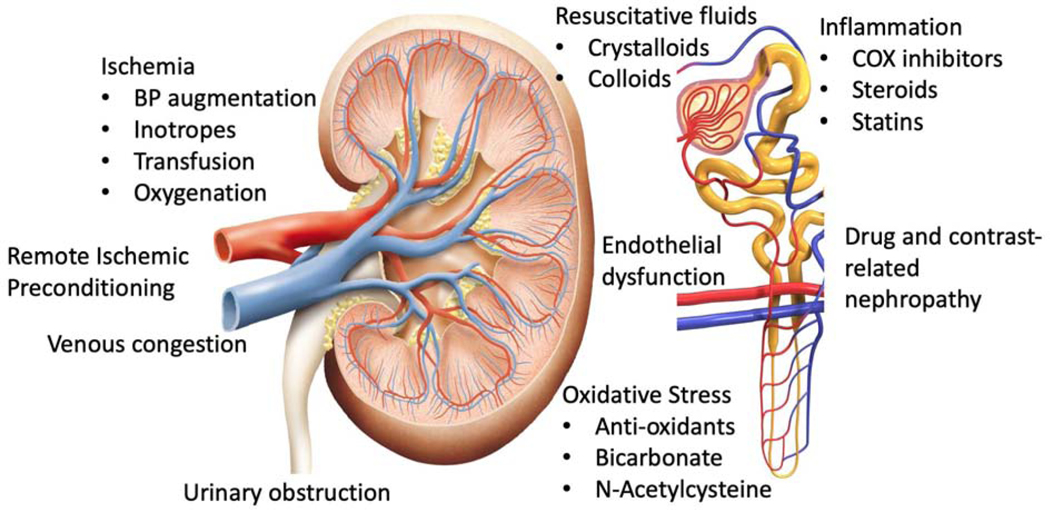
To characterize current evidence and current foci of perioperative clinical trials, we systematically reviewed Medline and identified perioperative trials involving 100 or more adult patients undergoing surgery and reporting renal end points that were published in high-impact journals since 2004. We categorized the 101 trials identified based on the nature of the intervention and summarized major trial findings from the five categories most applicable to perioperative management of patients. Trials that targeted ischemia suggested that increasing perioperative renal oxygen delivery with inotropes or blood transfusion does not reliably mitigate acute kidney injury (AKI), although goal-directed therapy with hemodynamic monitors appeared beneficial in some trials. Trials that have targeted inflammation or oxidative stress, including studies of nonsteroidal anti-inflammatory drugs, steroids, N-acetylcysteine, and sodium bicarbonate, have not shown renal benefits, and high-dose perioperative statin treatment increased AKI in some patient groups in two large trials. Balanced crystalloid intravenous fluids appear safer than saline, and crystalloids appear safer than colloids. Liberal compared with restrictive fluid administration reduced AKI in a recent large trial in open abdominal surgery. Remote ischemic preconditioning, although effective in several smaller trials, failed to reduce AKI in two larger trials. The translation of promising preclinical therapies to patients undergoing surgery remains poor, and most interventions that reduced perioperative AKI compared novel surgical management techniques or existing processes of care rather than novel pharmacologic interventions.
为了描述围手术期临床试验的当前证据和重点,我们系统地检索了 Medline,并确定了自 2004 年以来在高影响力期刊上发表的涉及 100 名或更多成年手术患者并报告肾脏终点的围手术期试验。我们根据干预的性质对 101 项试验进行了分类,并从最适用于患者围手术期管理的五类试验中总结了主要试验结果。针对缺血的试验表明,使用正性肌力药或输血增加围手术期肾脏氧输送并不能可靠地减轻急性肾损伤 (AKI),尽管使用血流动力学监测的目标导向治疗在一些试验中似乎有益。针对炎症或氧化应激的试验,包括非甾体抗炎药、类固醇、N-乙酰半胱氨酸和碳酸氢钠的研究,并未显示肾脏获益,并且在两项大型试验中,高剂量围手术期他汀类药物治疗增加了某些患者群体的 AKI。平衡晶体静脉输液似乎比生理盐水更安全,晶体液似乎比胶体液更安全。与限制性液体管理相比,自由液体管理在最近一项开放性腹部手术的大型试验中减少了 AKI。尽管在几项较小的试验中有效,但远程缺血预处理在两项较大的试验中未能降低 AKI。有前途的临床前治疗转化为接受手术的患者的效果仍然较差,与新型手术管理技术或现有护理流程相比,大多数减少围手术期 AKI 的干预措施都没有新型的药物干预措施。