Anesthesia and Intensive Care Unit, Department of Emergency and Organ Transplantation, University of Bari, Piazza G. Cesare, 11, 70124, Bari, Italy.
Crit Care. 2019 Jun 26;23(1):232. doi: 10.1186/s13054-019-2516-4.
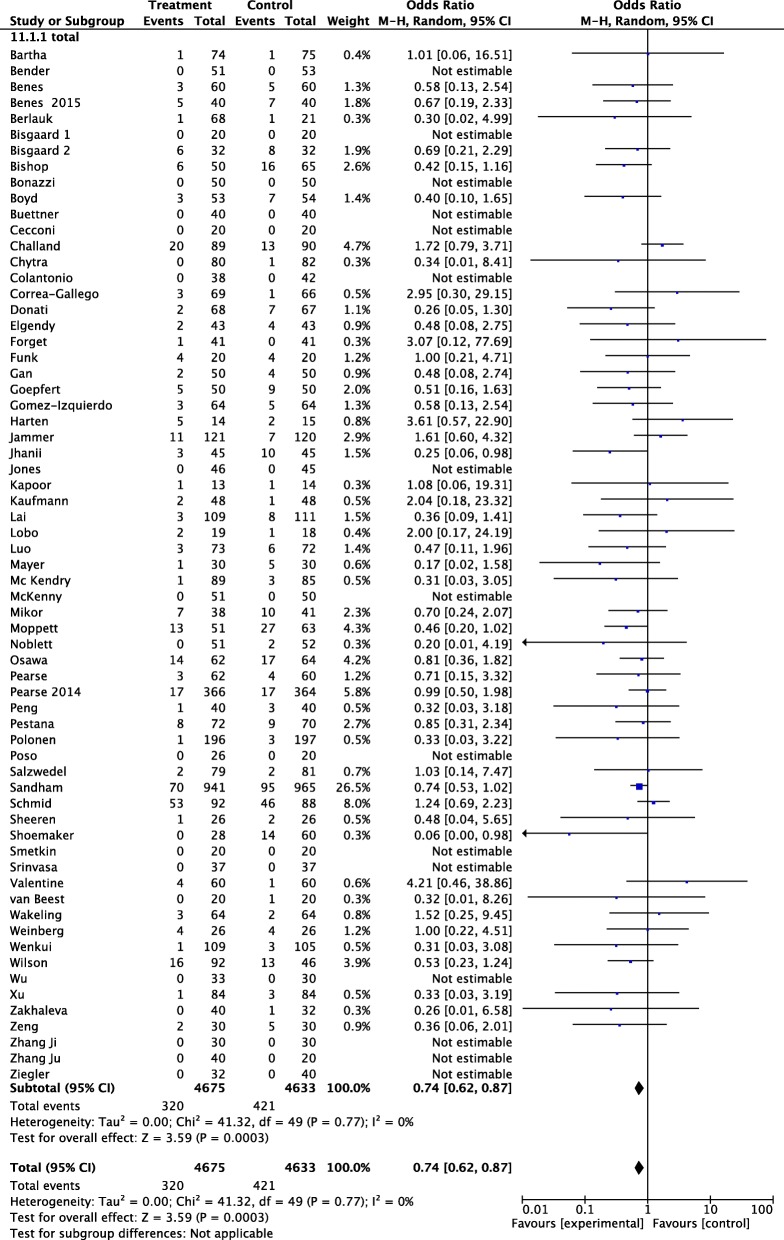
Perioperative goal-directed therapy (GDT) reduces the risk of renal injury. However, several questions remain unanswered, such as target, kind of patients and surgery, and role of fluids and inotropes. We therefore update a previous analysis, including all studies published in the meanwhile, to clarify the clinical impact of this strategy on acute kidney injury.
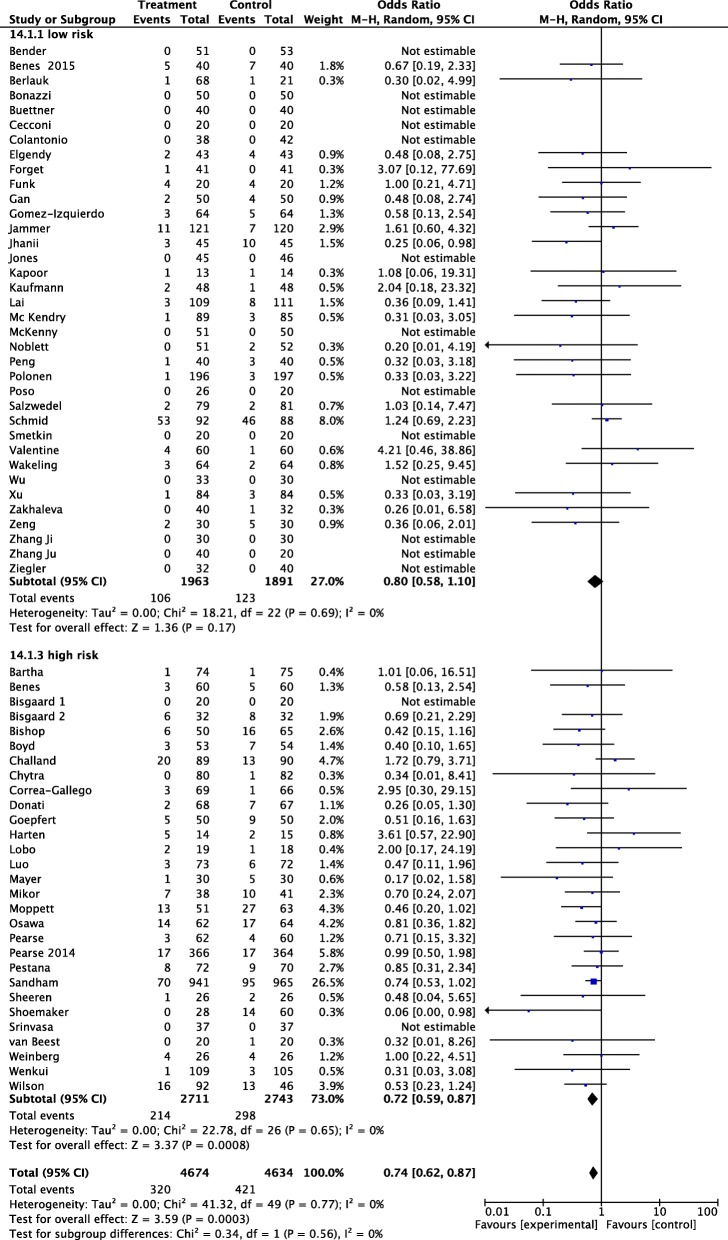
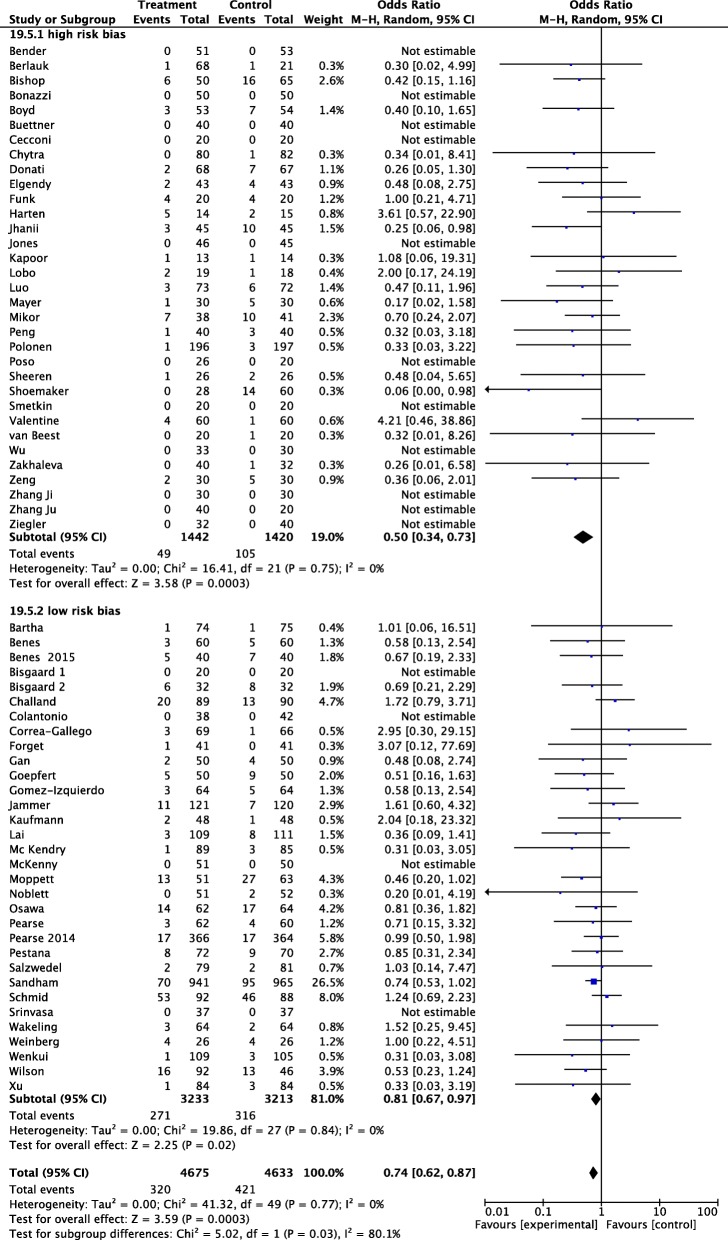
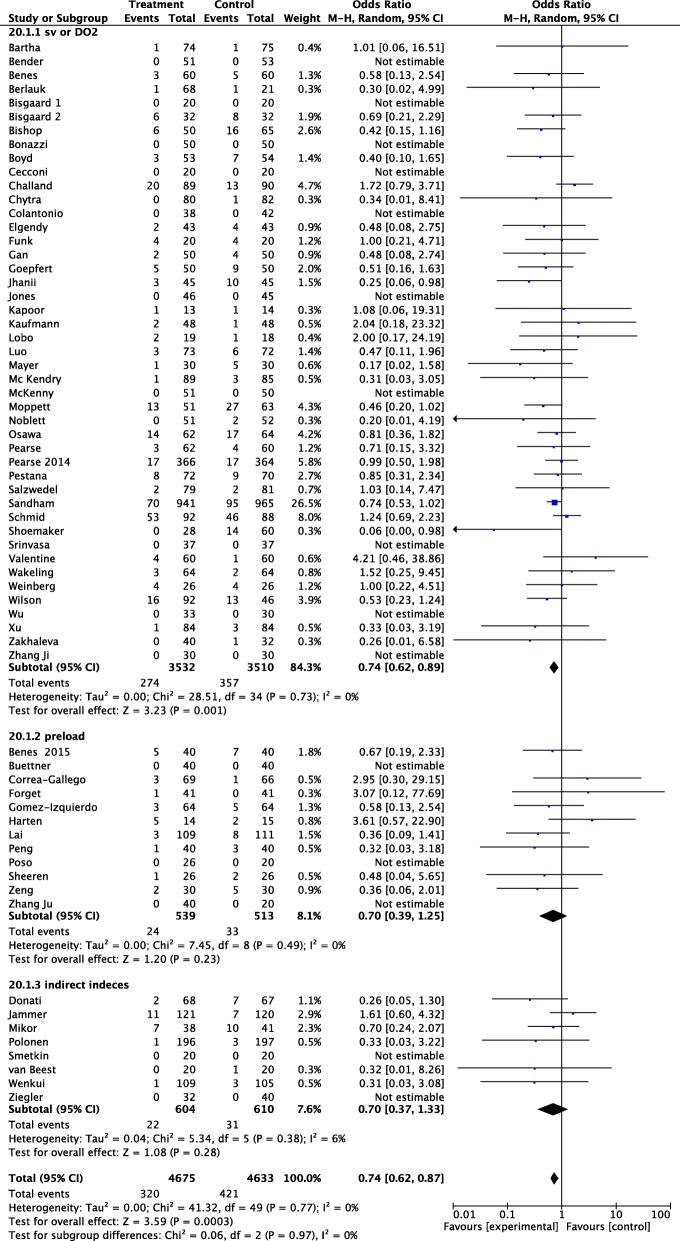
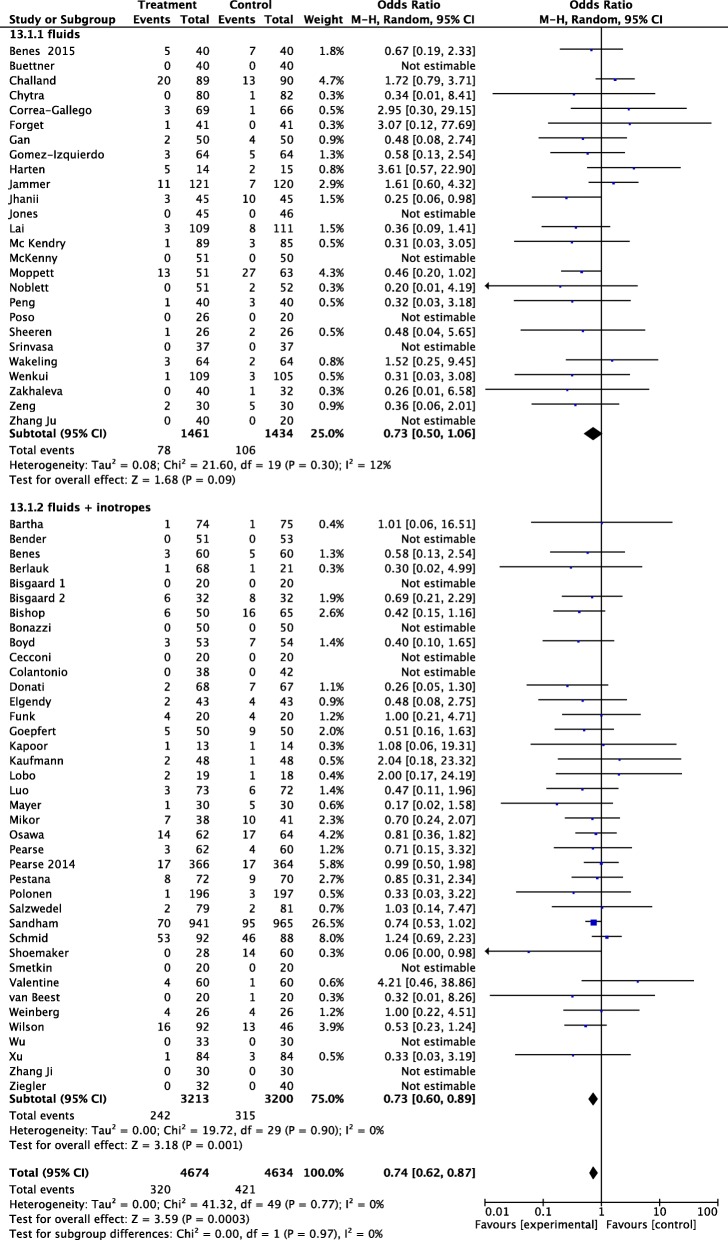
Randomized controlled trials enrolling adult patients undergoing major surgery were considered. GDT was defined as perioperative monitoring and manipulation of hemodynamic parameters to reach normal or supranormal values by fluids alone or with inotropes. Trials comparing the effects of GDT and standard hemodynamic therapy were considered. Primary outcome was acute kidney injury, whichever definition was used. Meta-analytic techniques (analysis software RevMan, version 5.3) were used to combine studies, using random-effect odds ratios (OR) and 95% confidence intervals (CI). Trial sequential analyses were performed including all trials and considering only low risk of bias trials. Sixty-five trials with an overall sample of 9308 patients were included. OR for the development of renal injury was 0.64 (95% CI, 0.62-0.87; p = 0.0003), with no statistical heterogeneity. Trial sequential analyses and sensitivity analysis including studies with low risk of bias confirmed the main results. A significant decrease in renal injury rate was observed in studies that adopted cardiac output and oxygen delivery as hemodynamic target and that used both fluids and inotropes. The postoperative kidney injury rate was significantly lower in trials enrolling "high-risk" patients and major abdominal and orthopedic surgery.
The present meta-analysis suggests that targeting GDT to perioperative systemic oxygen delivery, by means of fluids and inotropes, can be the best way to improve renal perfusion and oxygenation in high-risk patients undergoing major abdominal and orthopedic surgery.
围手术期目标导向治疗(GDT)可降低肾损伤风险。然而,仍有一些问题尚未得到解答,例如目标、患者类型和手术类型,以及液体和正性肌力药的作用。因此,我们更新了之前的分析,纳入了同时期发表的所有研究,以阐明该策略对急性肾损伤的临床影响。
纳入了接受大手术的成年患者的随机对照试验。GDT 被定义为围手术期监测和操纵血流动力学参数,通过单独使用液体或联合使用正性肌力药使血流动力学参数达到正常或高于正常水平。比较 GDT 和标准血流动力学治疗效果的试验被纳入。主要结局为急性肾损伤,无论采用何种定义。使用随机效应比值比(OR)和 95%置信区间(CI)对研究进行了荟萃分析(分析软件 RevMan,版本 5.3)。进行了试验序贯分析,包括所有试验,并仅考虑低偏倚风险的试验。纳入了 65 项试验,共有 9308 例患者。肾脏损伤发生率的 OR 为 0.64(95%CI,0.62-0.87;p=0.0003),无统计学异质性。试验序贯分析和包括低偏倚风险研究的敏感性分析证实了主要结果。观察到采用心输出量和氧输送作为血流动力学目标并同时使用液体和正性肌力药的研究中,肾脏损伤发生率显著降低。纳入“高危”患者和大腹部及骨科手术的试验中,术后肾脏损伤发生率显著降低。
本荟萃分析表明,通过液体和正性肌力药将 GDT 靶向围手术期全身氧输送,可能是改善高危患者大腹部和骨科手术中肾灌注和氧合的最佳方法。