Department of Urological Robotic Surgery and Renal Transplantation, Careggi Hospital, University of Florence, Florence, Italy; Department of Experimental and Clinical Medicine, University of Florence, Florence, Italy; Department of Urological Oncologic Minimally Invasive Robotic Surgery and Andrology, Careggi Hospital, University of Florence, Florence, Italy.
Division of Urology, Department of Oncology, School of Medicine, San Luigi Hospital, University of Turin, Orbassano, Turin, Italy.
Eur Urol. 2020 Jul;78(1):11-15. doi: 10.1016/j.eururo.2020.03.054. Epub 2020 Apr 11.
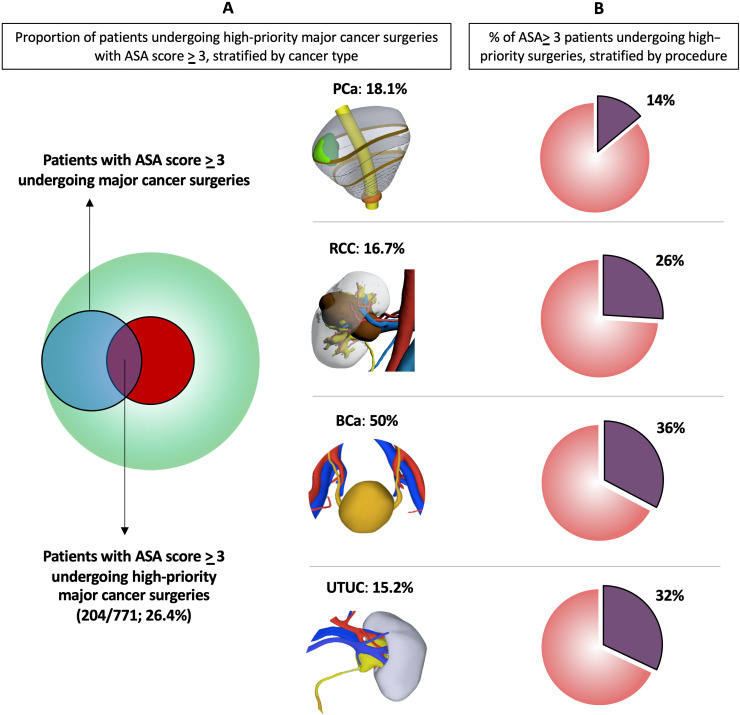
The coronavirus 2019 (COVID-19) pandemic has led to an unprecedented emergency scenario for all aspects of health care, including urology. At the time of writing, Italy was the country with the highest rates of both infection and mortality. A panel of experts recently released recommendations for prioritising urologic surgeries in a low-resource setting. Of note, major cancer surgery represents a compelling challenge. However, the burden of these procedures and the impact of such recommendations on urologic practice are currently unknown. To fill this gap, we assessed the yearly proportion of high-priority major uro-oncologic surgeries at three Italian high-volume academic centres. Of 2387 major cancer surgeries, 32.3% were classified as high priority (12.6% of radical nephroureterectomy, 17.3% of nephrectomy, 33.9% of radical prostatectomy, and 36.2% of radical cystectomy cases). Moreover, 26.4% of high-priority major cancer surgeries were performed in patients at higher perioperative risk (American Society of Anesthesiologists score ≥3), with radical cystectomy contributing the most to this cohort (50%). Our real-life data contextualise ongoing recommendations on prioritisation strategies during the current COVID-19 pandemic, highlighting the need for better patient selection for surgery. We found that approximately two-thirds of elective major uro-oncologic surgeries can be safely postponed or changed to another treatment modality when the availability of health care resources is reduced. PATIENT SUMMARY: We used data from three high-volume Italian academic urology centres to evaluate how many surgeries performed for prostate, bladder, kidney, and upper tract urothelial cancer can be postponed in times of emergency. We found that approximately two-thirds of patients with these cancers do not require high-priority surgery. Conversely, of patients requiring high-priority surgery, approximately one in four is considered at high perioperative risk. These patients may pose challenges in allocation of resources in critical scenarios such as the current COVID-19 pandemic.
2019 年冠状病毒病(COVID-19)大流行导致了医疗保健各个方面的空前紧急情况,包括泌尿科。在撰写本文时,意大利是感染率和死亡率最高的国家。一组专家最近发布了在资源有限的情况下对泌尿科手术进行优先排序的建议。值得注意的是,主要癌症手术是一个具有挑战性的问题。然而,这些手术的负担以及此类建议对泌尿科实践的影响尚不清楚。为了填补这一空白,我们评估了意大利三家高容量学术中心每年高优先级主要泌尿肿瘤手术的比例。在 2387 例主要癌症手术中,32.3%被归类为高优先级(根治性肾输尿管切除术占 12.6%,肾切除术占 17.3%,根治性前列腺切除术占 33.9%,根治性膀胱切除术占 36.2%)。此外,26.4%的高优先级主要癌症手术是在围手术期风险较高的患者中进行的(美国麻醉师协会评分≥3),其中根治性膀胱切除术对此类患者的贡献最大(50%)。我们的实际数据将当前 COVID-19 大流行期间的优先排序策略建议置于上下文中,突出了在医疗资源可用性降低时对手术进行更好的患者选择的必要性。我们发现,当卫生保健资源可用性降低时,可以安全地推迟或改变大约三分之二的择期主要泌尿肿瘤手术。
我们使用来自意大利三家高容量学术泌尿科中心的数据来评估在紧急情况下可以为前列腺癌、膀胱癌、肾癌和上尿路尿路上皮癌患者进行多少手术。我们发现,大约三分之二的这些癌症患者不需要高优先级手术。相反,需要高优先级手术的患者中,大约四分之一被认为处于高围手术期风险中。在当前 COVID-19 大流行等危急情况下,这些患者可能会对资源分配提出挑战。