Florescu Diana Ruxandra, Nistor Diana Elena
Faculty of Medicine, Carol Davila University of Medicine and Pharmacy, Bucharest, Romania.
Discoveries (Craiova). 2019 Mar 31;7(1):e89. doi: 10.15190/d.2019.2.
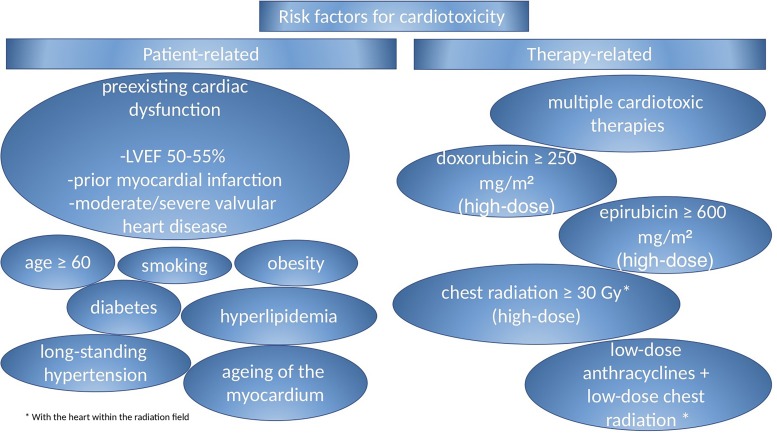
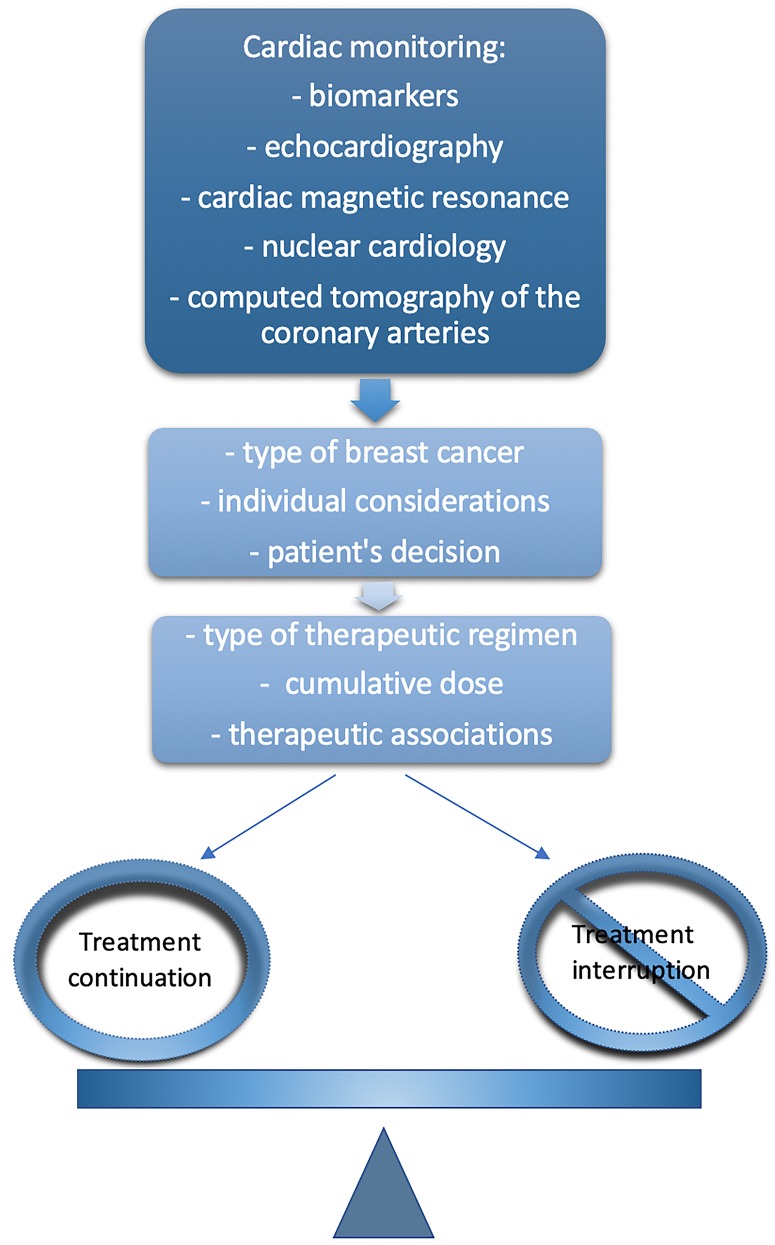
Breast cancer is the second most commonly diagnosed cancer, being one of the main health issues that needs to be addressed worldwide. New therapies have led to a remarkable increase in survival rates, which is unfortunately overshadowed by their negative impact on cardiac structure and function in disease-free patients. Since anthracyclines and trastuzumab cause the most undesired outcome in breast cancer patients - cardiac-related mortality, they have been widely studied. However, other therapies (such as hormonal therapy, tyrosine kinase inhibitors, anti-VEGF drugs etc.) can also affect the cardiovascular system and lead to ischemia, hypertension or vascular thromboembolism. Even though excessive research has been conducted in thepast decades, there are still no guidelines regarding the most adequate methods neither to detect and prevent severe cardiotoxicity that can finally lead to heart failure and ultimately death nor for the further management of patients after cardiotoxicity is detected. Biomarkers of ischemia (troponins T and I) and of overload (BNP and NT-proBNP) in association with periodic echocardiographies (assessment of the global longitudinal strain) are two of the most important means used by physicians in the evaluation of cardiac disease in this group of patients. Given that no internationally accepted guidelines for screening and surveillance of different populations exist, the cardio-oncology team is crucial in the management of these patients, their collaboration resulting in individualized treatment regimens. After careful evaluation of different variables (treatment effects, malignancy status, and the patient's pre-existing conditions), a decision is made to either reduce the dosage or rate of administration, change the medication or interrupt the treatment and initiate the cardioprotective therapeutic associations. Consequently, it is an absolute necessity the development of customized treatment guidelines and the conduction of multiple clinical studies in order to demonstrate their effect on long-term survival.
乳腺癌是第二大最常被诊断出的癌症,是全球范围内需要解决的主要健康问题之一。新疗法使生存率显著提高,但遗憾的是,其对无病患者心脏结构和功能的负面影响却使其黯然失色。由于蒽环类药物和曲妥珠单抗在乳腺癌患者中导致了最不理想的结果——心脏相关死亡率,因此对它们进行了广泛研究。然而,其他疗法(如激素疗法、酪氨酸激酶抑制剂、抗血管内皮生长因子药物等)也会影响心血管系统,导致缺血、高血压或血管血栓栓塞。尽管在过去几十年里进行了大量研究,但对于检测和预防最终可能导致心力衰竭乃至死亡的严重心脏毒性的最适当方法,以及在检测到心脏毒性后对患者的进一步管理,仍然没有相关指南。缺血生物标志物(肌钙蛋白T和I)和超负荷生物标志物(脑钠肽和N末端脑钠肽原)与定期超声心动图检查(整体纵向应变评估)是医生评估这类患者心脏疾病时最重要的两种手段。鉴于不存在针对不同人群筛查和监测的国际公认指南,心脏肿瘤学团队在管理这些患者方面至关重要,他们的合作会产生个性化的治疗方案。在仔细评估不同变量(治疗效果、恶性肿瘤状态和患者的既往病史)后,决定是降低给药剂量或速率、更换药物、中断治疗还是启动心脏保护治疗联合方案。因此,制定定制化治疗指南并开展多项临床研究以证明其对长期生存的影响是绝对必要的。