Department of Blood Transfusion and Cell Therapy, Ehime University Hospital, Toon, Ehime, Japan.
Center for Basic Medical Research, International University of Health and Welfare, Otawara, Tochigi, Japan.
Blood Adv. 2020 Apr 28;4(8):1648-1655. doi: 10.1182/bloodadvances.2020001446.
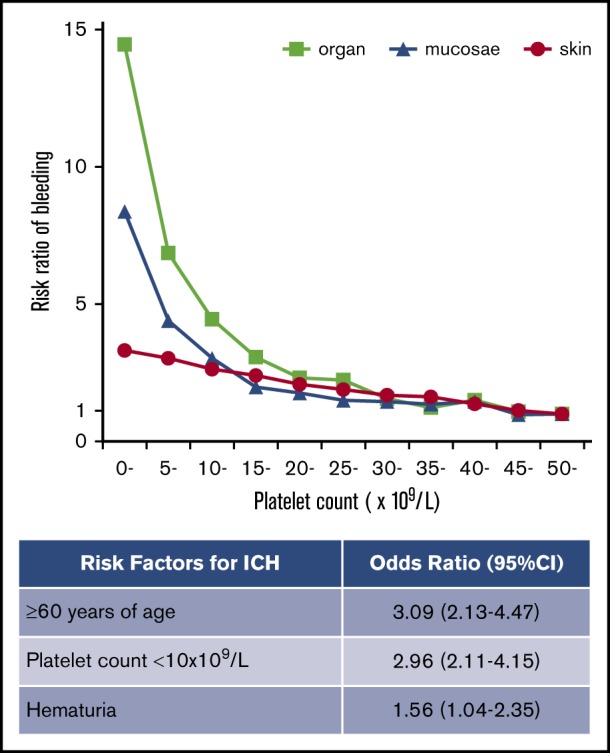
Bleeding manifestations in primary immune thrombocytopenia (ITP) range from skin petechiae to life-threatening intracranial hemorrhage (ICH). However, the relation between these various bleeding manifestations and the platelet count in ITP remains poorly characterized. Using a nationwide database of patients with ITP during the years 2005 to 2014 (10 years) in Japan, we analyzed 19 415 adult patients newly diagnosed with ITP, including 222 with ICH. The frequency of skin purpura was 64.8%, and this increased linearly with thrombocytopenia without a specific platelet count threshold. In contrast, mucosal bleeding (epistaxis and gingival bleeding) and organ bleeding (melena, hematuria, and ICH) increased exponentially with thrombocytopenia at a platelet count threshold of 10 to 15 × 109/L. Age showed a much weaker correlation than platelet count with skin and mucosal bleeding. However, the incidence of organ bleeding increased exponentially above 60 years of age. Multivariate analysis showed that the presence of mucosal bleeding was a risk factor for occurrence of melena and hematuria but not for ICH. The frequency of ICH was 1.1% and risk factors for ICH were age ≥60 years (odds ratio [OR], 3.09; 95% confidence interval [CI], 2.13-4.47; P < .001), platelet count <10 × 109/L (OR, 2.96; 95% CI, 2.11-4.15; P < .001), and the presence of hematuria (OR, 1.56; 95% CI, 1.04-2.35; P = .033). The relation between ICH and platelet count varied with age. This large-scale analysis of risk factors for bleeding in ITP has revealed distinct characteristics of skin, mucosal, and organ bleeding in adult patients with newly diagnosed ITP, thus indicating those who are at a high risk of severe organ bleeding.
原发性免疫性血小板减少症 (ITP) 的出血表现范围从皮肤瘀点到危及生命的颅内出血 (ICH)。然而,这些不同的出血表现与 ITP 中的血小板计数之间的关系仍未得到很好的描述。利用日本 2005 年至 2014 年 (10 年) 期间的 ITP 患者全国性数据库,我们分析了 19415 例新诊断为 ITP 的成年患者,其中包括 222 例 ICH 患者。皮肤紫癜的发生率为 64.8%,并且随着血小板减少呈线性增加,没有特定的血小板计数阈值。相比之下,黏膜出血(鼻出血和牙龈出血)和器官出血(黑便、血尿和 ICH)随着血小板计数在 10 到 15×109/L 的阈值呈指数增加。年龄与皮肤和黏膜出血的相关性远弱于血小板计数。然而,器官出血的发生率在 60 岁以上呈指数增加。多变量分析显示,黏膜出血的存在是发生黑便和血尿的危险因素,但不是 ICH 的危险因素。ICH 的发生率为 1.1%,ICH 的危险因素是年龄≥60 岁(比值比 [OR],3.09;95%置信区间 [CI],2.13-4.47;P<0.001),血小板计数<10×109/L(OR,2.96;95% CI,2.11-4.15;P<0.001),以及血尿的存在(OR,1.56;95% CI,1.04-2.35;P=0.033)。ICH 与血小板计数之间的关系随年龄而变化。对 ITP 出血危险因素的这项大规模分析揭示了新诊断为 ITP 的成年患者皮肤、黏膜和器官出血的明显特征,从而表明那些有发生严重器官出血高风险的患者。