Department of Epidemiology, Tulane University School of Public Health and Tropical Medicine, 1440 Canal Street, Suite 2000, New Orleans, Louisiana, 70112, USA.
Department of Medicine, Tulane University School of Medicine, New Orleans, Louisiana, USA.
BMC Cardiovasc Disord. 2020 Apr 25;20(1):202. doi: 10.1186/s12872-020-01485-2.
Heart failure (HF) represents an accumulated burden of systemic vascular damage and is the fastest growing form of cardiovascular disease (CVD). Due to increasing HF-attributable mortality rates, we sought to assess the association of the new 2019 Pooled Cohort equations to Prevent Heart Failure (PCP-HF) risk score with CVD and all-cause mortality.
We linked data for 6333 black and white men and women aged 40-79 years, whom underwent electrocardiographic examination from the Third National Health and Nutrition Exam Survey, to National Death Index record matches. Sex- and race-specific PCP-HF risk scores were calculated using data on age, smoking, body mass index, systolic blood pressure, total cholesterol, HDL-cholesterol, fasting blood glucose, QRS complex duration, and antihypertensive and/or glucose-lowering medications. Cox regression estimated hazard ratios for the association of the PCP-HF risk score with CVD and all-cause mortality.
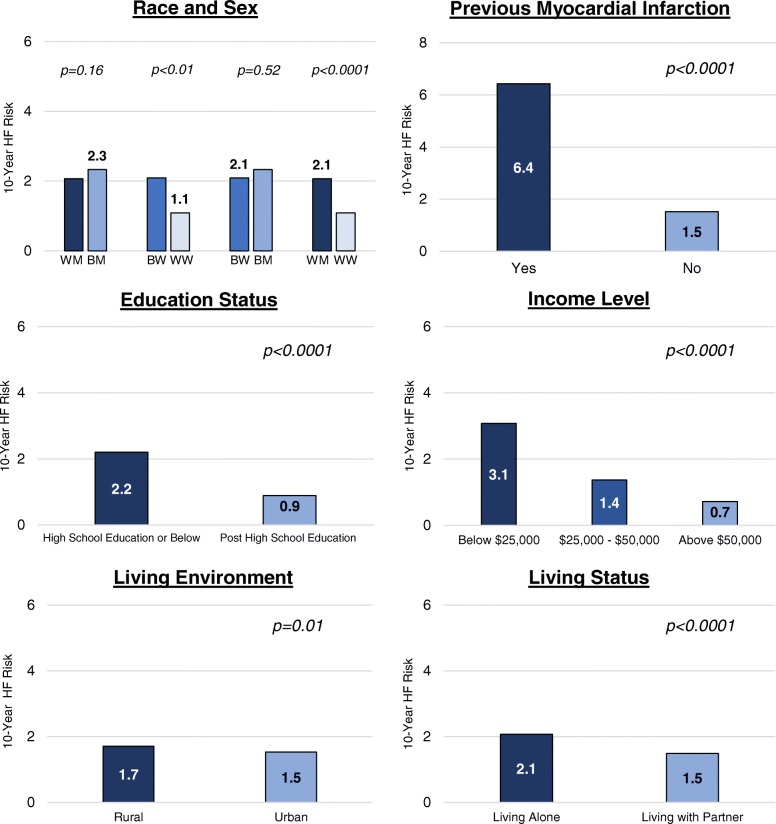
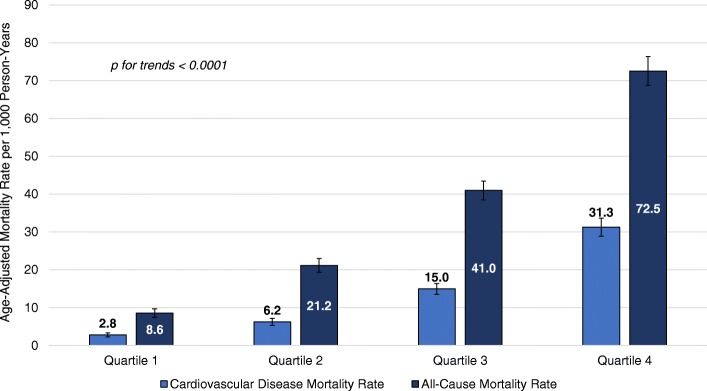
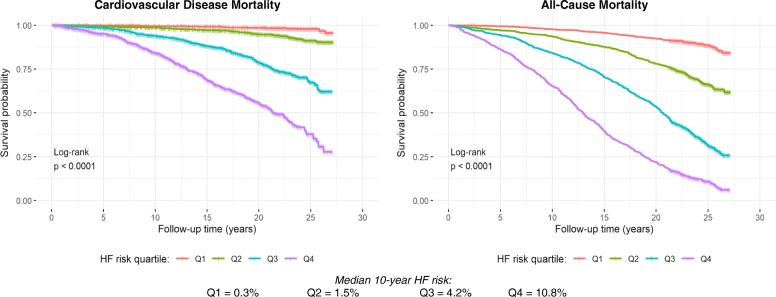
Individuals were on average 54.9 years old (51.7% women, 25.4% black) and the median 10-year HF risk was 1.6% (Q1 = 0.5, Q3 = 4.8). There were 3178 deaths, 1116 from CVD, over a median follow-up time of 22.3 years. Black women had a higher 10-year HF risk compared to white women (2.1% vs. 1.1%; p < 0.01), while no significant difference was observed in predicted HF risk between black men and white men (2.3% vs. 2.1%, p = 0.16). A two-fold higher PCP-HF risk score was associated with a significant 58% (HR = 1.58; 95% CI, 1.48-1.70; p < 0.0001) and 38% (HR = 1.38; 95% CI, 1.32-1.46; p < 0.0001) greater risk of CVD and all-cause mortality, respectively.
The PCP-HF risk score predicts CVD and all-cause mortality, in addition to the 10-year risk of incident HF among white and black men and women. These results underline the expanded utility of the PCP-HF risk score and suggest that its implementation in the clinical and population health settings may improve primary CVD prevention in the United States.
心力衰竭(HF)代表了全身血管损伤的累积负担,是心血管疾病(CVD)中增长最快的形式。由于 HF 相关死亡率的增加,我们试图评估新的 2019 年用于预防心力衰竭(PCP-HF)的 pooled cohort 方程与 CVD 和全因死亡率的相关性。
我们将第三项全国健康和营养检查调查中接受心电图检查的 6333 名黑人和白人年龄在 40-79 岁的男女的数据与国家死亡指数记录相匹配。使用年龄、吸烟、体重指数、收缩压、总胆固醇、高密度脂蛋白胆固醇、空腹血糖、QRS 复合波持续时间以及降压和/或降糖药物的数据,计算出男女特定的 PCP-HF 风险评分。Cox 回归估计了 PCP-HF 风险评分与 CVD 和全因死亡率的相关性。
参与者平均年龄为 54.9 岁(51.7%为女性,25.4%为黑人),中位 10 年 HF 风险为 1.6%(Q1=0.5,Q3=4.8)。中位随访时间为 22.3 年,共有 3178 人死亡,1116 人死于 CVD。黑人女性的 10 年 HF 风险高于白人女性(2.1%比 1.1%;p<0.01),而黑人男性和白人男性之间的 HF 风险预测值无显著差异(2.3%比 2.1%;p=0.16)。两倍的 PCP-HF 风险评分与 CVD 和全因死亡率的显著风险增加 58%(HR=1.58;95%CI,1.48-1.70;p<0.0001)和 38%(HR=1.38;95%CI,1.32-1.46;p<0.0001)相关。
PCP-HF 风险评分可预测 CVD 和全因死亡率,此外还可预测白人和黑人男女中 HF 事件的 10 年风险。这些结果强调了 PCP-HF 风险评分的扩展用途,并表明在美国,其在临床和人群健康环境中的实施可能会改善 CVD 的一级预防。