Department of Epidemiology, School of Public Health, University of Alabama at Birmingham, AL
Department of Surgery, School of Medicine, University of Alabama at Birmingham, AL.
J Am Heart Assoc. 2017 Mar 17;6(3):e005676. doi: 10.1161/JAHA.117.005676.
The atherosclerosis cardiovascular disease (ASCVD) Pooled Cohort risk equations have shown different calibration across US populations with varied levels of social deprivation.
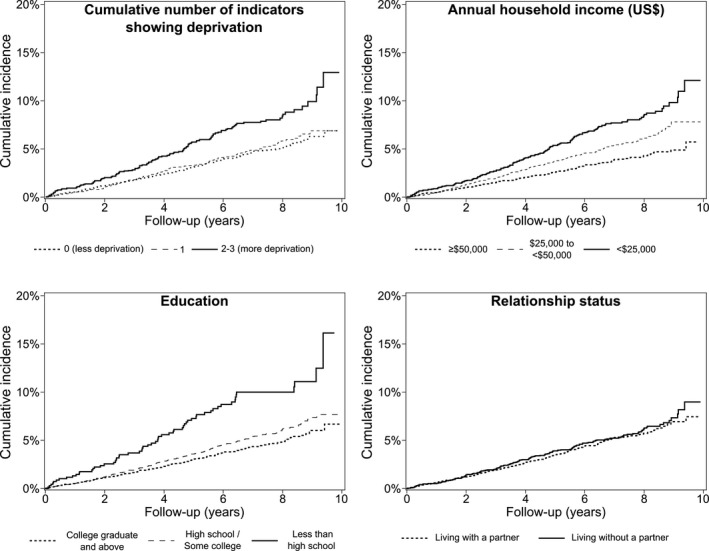
We analyzed the calibration and discrimination of the Pooled Cohort risk equations by social deprivation status among 9066 REGARDS (REasons for Geographic And Racial Differences in Stroke) study participants not taking statins for whom ASCVD risk may lead to statin initiation. Patients were aged 45 to 79 years, had no ASCVD or diabetes mellitus, and had a low-density lipoprotein cholesterol level 70 to 189 mg/dL. Social deprivation was defined using 3 indicators: annual household income <$25 000, less than a high school education, and living without a partner. At baseline in 2003-2007, 54.6%, 27.4%, and 18.0% of participants had 0, 1, and 2 or 3 indicators showing deprivation, respectively. From baseline through December 2012, 457 participants developed ASCVD (nonfatal/fatal stroke, myocardial infarction, or coronary heart disease death). Predicted and observed ASCVD incidence per 1000 person-years were 8.02 and 6.23 (95% CI, 5.31-7.31), respectively, among participants with 0 indicators of deprivation (Hosmer-Lemeshow =0.01); 8.05 and 6.61 (95% CI, 5.29-8.24), respectively, with 1 indicator (=0.09); and 9.83 and 11.40 (95% CI, 9.23-14.05), respectively, with 2 or 3 indicators (=0.12). The C-index (95% CI) was 0.72 (0.69-0.75), 0.73 (0.69-0.78), and 0.70 (0.65-0.75) among participants with 0, 1, and 2 or 3 indicators of deprivation, respectively. The net reclassification improvement after adding deprivation data to the Pooled Cohort risk equations was modest (0.12; 95% CI, 0.03-0.21).
The Pooled Cohort risk equations have good calibration among individuals with social deprivation but overestimate ASCVD risk among those with less social deprivation.
动脉粥样硬化性心血管疾病(ASCVD)的汇总队列风险方程在社会剥夺程度不同的美国人群中表现出不同的校准。
我们在 9066 名 REGARDS(地理和种族差异中风原因)研究参与者中分析了汇总队列风险方程按社会剥夺状态的校准和区分,这些参与者未服用他汀类药物,ASCVD 风险可能导致开始使用他汀类药物。患者年龄在 45 至 79 岁之间,无 ASCVD 或糖尿病,且低密度脂蛋白胆固醇水平为 70 至 189mg/dL。社会剥夺程度使用 3 个指标定义:家庭年收入<25000 美元、未接受过高中教育以及没有伴侣。在 2003-2007 年的基线时,分别有 54.6%、27.4%和 18.0%的参与者有 0、1 和 2 或 3 个显示剥夺的指标。截至 2012 年 12 月,有 457 名参与者发生 ASCVD(非致命/致命性中风、心肌梗死或冠心病死亡)。无剥夺指标的参与者每 1000 人年的预测和观察到的 ASCVD 发生率分别为 8.02 和 6.23(95%CI,5.31-7.31)(Hosmer-Lemeshow=0.01);分别有 1 个指标的发生率分别为 8.05 和 6.61(95%CI,5.29-8.24)(Hosmer-Lemeshow=0.09);有 2 或 3 个指标的发生率分别为 9.83 和 11.40(95%CI,9.23-14.05)(Hosmer-Lemeshow=0.12)。无剥夺指标的参与者的 C 指数(95%CI)分别为 0.72(0.69-0.75)、0.73(0.69-0.78)和 0.70(0.65-0.75)。在有 0、1 和 2 或 3 个社会剥夺指标的参与者中,分别为 0.12(95%CI,0.03-0.21)。
汇总队列风险方程在社会弱势群体中具有良好的校准性,但在社会弱势群体中高估了 ASCVD 风险。