Fondazione Umbra Cuore e Ipertensione-ONLUS and Struttura Complessa di Cardiologia, Ospedale S. Maria della Misericordia, Perugia..
Fondazione Umbra Cuore e Ipertensione-ONLUS and Struttura Complessa di Cardiologia, Ospedale S. Maria della Misericordia, Perugia.
Eur J Intern Med. 2020 Jun;76:14-20. doi: 10.1016/j.ejim.2020.04.037. Epub 2020 Apr 20.
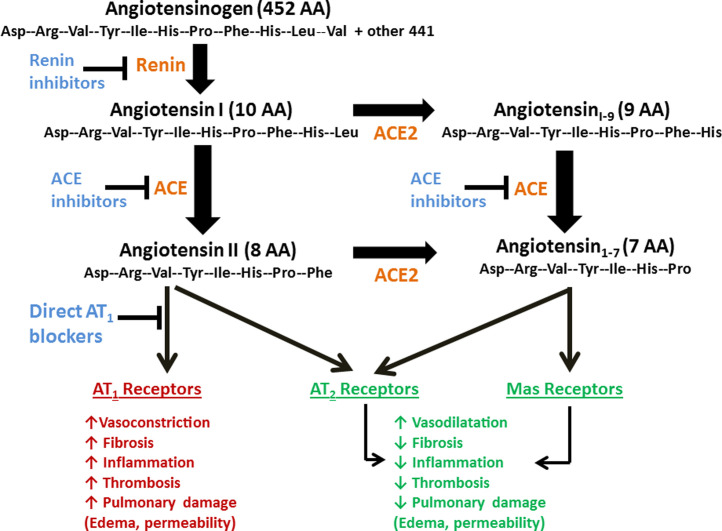
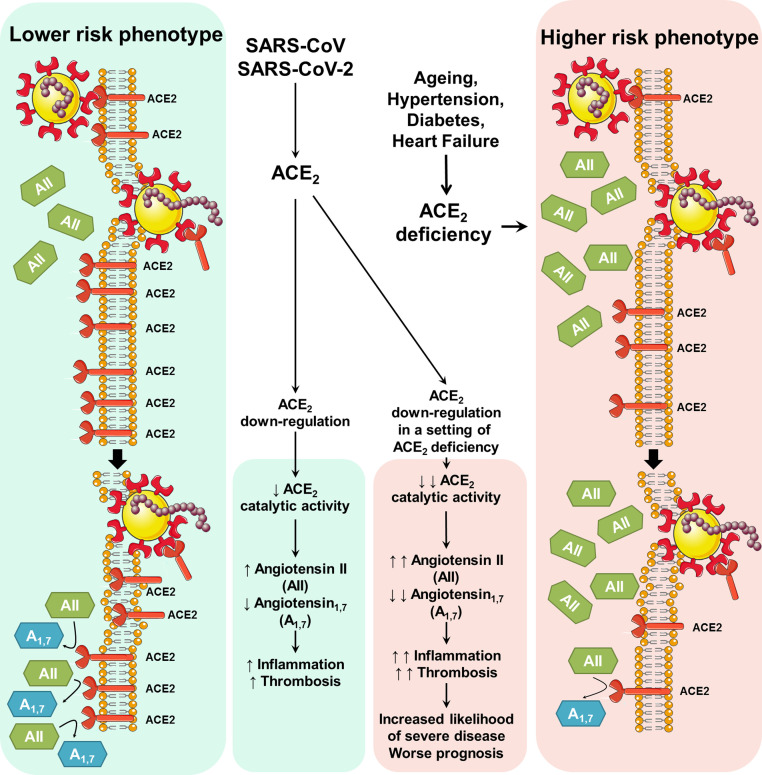
Angiotensin converting enzyme-2 (ACE2) receptors mediate the entry into the cell of three strains of coronavirus: SARS-CoV, NL63 and SARS-CoV-2. ACE2 receptors are ubiquitous and widely expressed in the heart, vessels, gut, lung (particularly in type 2 pneumocytes and macrophages), kidney, testis and brain. ACE2 is mostly bound to cell membranes and only scarcely present in the circulation in a soluble form. An important salutary function of membrane-bound and soluble ACE2 is the degradation of angiotensin II to angiotensin. Consequently, ACE2 receptors limit several detrimental effects resulting from binding of angiotensin II to AT1 receptors, which include vasoconstriction, enhanced inflammation and thrombosis. The increased generation of angiotensin also triggers counter-regulatory protective effects through binding to G-protein coupled Mas receptors. Unfortunately, the entry of SARS-CoV2 into the cells through membrane fusion markedly down-regulates ACE2 receptors, with loss of the catalytic effect of these receptors at the external site of the membrane. Increased pulmonary inflammation and coagulation have been reported as unwanted effects of enhanced and unopposed angiotensin II effects via the ACE→Angiotensin II→AT1 receptor axis. Clinical reports of patients infected with SARS-CoV-2 show that several features associated with infection and severity of the disease (i.e., older age, hypertension, diabetes, cardiovascular disease) share a variable degree of ACE2 deficiency. We suggest that ACE2 down-regulation induced by viral invasion may be especially detrimental in people with baseline ACE2 deficiency associated with the above conditions. The additional ACE2 deficiency after viral invasion might amplify the dysregulation between the 'adverse' ACE→Angiotensin II→AT1 receptor axis and the 'protective' ACE2→Angiotensin→Mas receptor axis. In the lungs, such dysregulation would favor the progression of inflammatory and thrombotic processes triggered by local angiotensin II hyperactivity unopposed by angiotensin. In this setting, recombinant ACE2, angiotensin and angiotensin II type 1 receptor blockers could be promising therapeutic approaches in patients with SARS-CoV-2 infection.
血管紧张素转换酶 2(ACE2)受体介导三种冠状病毒:SARS-CoV、NL63 和 SARS-CoV-2 进入细胞。ACE2 受体广泛存在并在心脏、血管、肠道、肺(特别是 2 型肺泡细胞和巨噬细胞)、肾脏、睾丸和大脑中广泛表达。ACE2 主要与细胞膜结合,只有很少一部分以可溶性形式存在于循环中。膜结合和可溶性 ACE2 的一个重要有益功能是将血管紧张素 II 降解为血管紧张素。因此,ACE2 受体限制了血管紧张素 II 与 AT1 受体结合引起的几种有害作用,包括血管收缩、炎症增强和血栓形成。血管紧张素的产生增加也会通过与 G 蛋白偶联的 Mas 受体结合触发代偿性保护作用。不幸的是,SARS-CoV-2 通过膜融合进入细胞会显著下调 ACE2 受体,导致这些受体在膜外部位的催化作用丧失。据报道,增强和不受抑制的血管紧张素 II 通过 ACE→血管紧张素 II→AT1 受体轴的作用会导致肺部炎症和凝血增加,这是不希望出现的副作用。感染 SARS-CoV-2 的患者的临床报告显示,与感染和疾病严重程度相关的几个特征(即年龄较大、高血压、糖尿病、心血管疾病)与 ACE2 缺乏程度不同。我们认为,病毒入侵引起的 ACE2 下调可能对伴有上述疾病的基线 ACE2 缺乏的人尤其有害。病毒入侵后 ACE2 缺乏的增加可能会放大“不利”ACE→血管紧张素 II→AT1 受体轴和“保护”ACE2→血管紧张素→Mas 受体轴之间的失调。在肺部,这种失调会有利于局部血管紧张素 II 活性增加而不受血管紧张素抑制引起的炎症和血栓形成过程的进展。在这种情况下,重组 ACE2、血管紧张素和血管紧张素 II 型 1 受体阻滞剂可能是 SARS-CoV-2 感染患者有前途的治疗方法。