Department of Pediatrics, All India Institute of Medical Sciences, New Delhi, 110029, India.
Indian J Pediatr. 2020 Jun;87(6):433-442. doi: 10.1007/s12098-020-03292-1. Epub 2020 Apr 27.
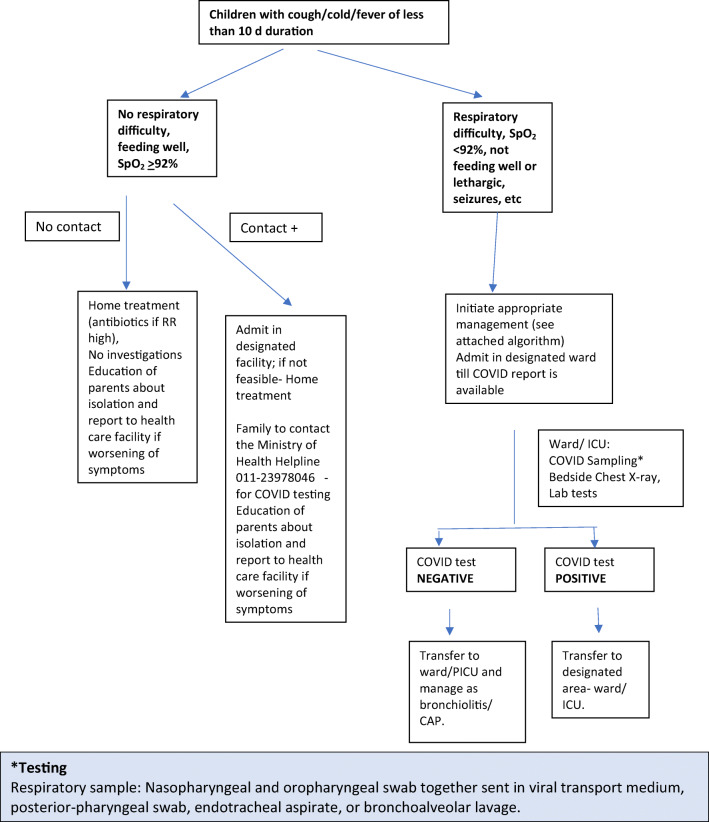
COVID-19 pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a major public health crisis threatening humanity at this point in time. Transmission of the infection occurs by inhalation of infected droplets or direct contact with soiled surfaces and fomites. It should be suspected in all symptomatic children who have undertaken international travel in the last 14 d, all hospitalized children with severe acute respiratory illness, and asymptomatic direct and high-risk contacts of a confirmed case. Clinical symptoms are similar to any acute respiratory viral infection with less pronounced nasal symptoms. Disease seems to be milder in children, but situation appears to be changing. Infants and young children had relatively more severe illness than older children. The case fatality rate is low in children. Diagnosis can be confirmed by Reverse transcriptase - Polymerase chain reaction (RT-PCR) on respiratory specimen (commonly nasopharyngeal and oropharyngeal swab). Rapid progress is being made to develop rapid diagnostic tests, which will help ramp up the capacity to test and also reduce the time to getting test results. Management is mainly supportive care. In severe pneumonia and critically ill children, trial of hydroxychloroquine or lopinavir/ritonavir should be considered. As per current policy, children with mild disease also need to be hospitalized; if this is not feasible, these children may be managed on ambulatory basis with strict home isolation. Pneumonia, severe disease and critical illness require admission and aggressive management for acute lung injury and shock and/or multiorgan dysfunction, if present. An early intubation is preferred over non-invasive ventilation or heated, humidified, high flow nasal cannula oxygen, as these may generate aerosols increasing the risk of infection in health care personnel. To prevent post discharge dissemination of infection, home isolation for 1-2 wk may be advised. As of now, no vaccine or specific chemotherapeutic agents are approved for children.
由严重急性呼吸系统综合症冠状病毒 2(SARS-CoV-2)引起的 COVID-19 大流行是目前威胁人类的重大公共卫生危机。感染通过吸入受感染的飞沫或直接接触受污染的表面和污染物传播。在过去 14 天内有国际旅行史的所有有症状的儿童、所有因严重急性呼吸道疾病住院的儿童以及确诊病例的无症状直接和高风险接触者,都应怀疑感染了这种疾病。临床症状与任何急性呼吸道病毒感染相似,鼻部症状不太明显。这种疾病在儿童中似乎较轻,但情况似乎正在发生变化。婴儿和幼儿的病情比年长儿童相对更严重。儿童的病死率较低。通过呼吸道标本(通常为鼻咽和口咽拭子)的逆转录酶-聚合酶链反应(RT-PCR)可以确诊。正在迅速开发快速诊断测试,这将有助于提高测试能力,并减少获得测试结果的时间。治疗主要是支持性治疗。在严重肺炎和危重症儿童中,应考虑试用羟氯喹或洛匹那韦/利托那韦。根据现行政策,轻症患儿也需要住院治疗;如果不可行,这些患儿可以在严格居家隔离的情况下进行门诊管理。如果出现肺炎、严重疾病和危重症,需要入院并积极治疗急性肺损伤和休克以及/或多器官功能障碍。如果存在这些情况,应首选气管插管,而不是无创通气或加热、湿化、高流量鼻导管吸氧,因为这些方法可能会产生气溶胶,增加医务人员感染的风险。为防止出院后传播感染,建议在家中隔离 1-2 周。到目前为止,还没有批准用于儿童的疫苗或特定的化疗药物。