Murray Marylou, Hine Paul
Department of Clinical Sciences, Liverpool School of Tropical Medicine, Liverpool, UK.
Cochrane Database Syst Rev. 2020 Apr 28;4(4):CD013594. doi: 10.1002/14651858.CD013594.
Progressive disseminated histoplasmosis (PDH) is a serious fungal infection that affects people living with HIV. The best way to treat the condition is unclear.
We assessed evidence in three areas of equipoise. 1. Induction. To compare efficacy and safety of initial therapy with liposomal amphotericin B versus initial therapy with alternative antifungals. 2. Maintenance. To compare efficacy and safety of maintenance therapy with 12 months of oral antifungal treatment with shorter durations of maintenance therapy. 3. Antiretroviral therapy (ART). To compare the outcomes of early initiation versus delayed initiation of ART.
We searched the Cochrane Infectious Diseases Group Specialized Register; Cochrane CENTRAL; MEDLINE (PubMed); Embase (Ovid); Science Citation Index Expanded, Conference Proceedings Citation Index-Science, and BIOSIS Previews (all three in the Web of Science); the WHO International Clinical Trials Registry Platform, ClinicalTrials.gov, and the ISRCTN registry, all up to 20 March 2020.
We evaluated studies assessing the use of liposomal amphotericin B and alternative antifungals for induction therapy; studies assessing the duration of antifungals for maintenance therapy; and studies assessing the timing of ART. We included randomized controlled trials (RCT), single-arm trials, prospective cohort studies, and single-arm cohort studies.
Two review authors assessed eligibility and risk of bias, extracted data, and assessed certainty of evidence. We used the Cochrane 'Risk of bias' tool to assess risk of bias in randomized studies, and ROBINS-I tool to assess risk of bias in non-randomized studies. We summarized dichotomous outcomes using risk ratios (RRs), with 95% confidence intervals (CI).
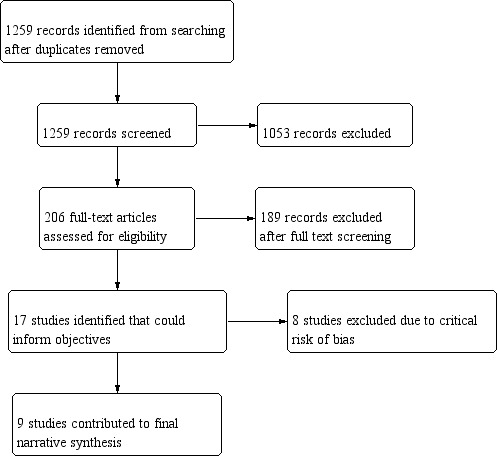
We identified 17 individual studies. We judged eight studies to be at critical risk of bias, and removed these from the analysis. 1. Induction We found one RCT which compared liposomal amphotericin B to deoxycholate amphotericin B. Compared to deoxycholate amphotericin B, liposomal amphotericin B may have higher clinical success rates (RR 1.46, 95% CI 1.01 to 2.11; 1 study, 80 participants; low-certainty evidence). Compared to deoxycholate amphotericin B, liposomal amphotericin B has lower rates of nephrotoxicity (RR 0.25, 95% CI 0.09 to 0.67; 1 study, 77 participants; high-certainty evidence). We found very low-certainty evidence to inform comparisons between amphotericin B formulations and azoles for induction therapy. 2. Maintenance We found no eligible study that compared less than 12 months of oral antifungal treatment to 12 months or greater for maintenance therapy. For both induction and maintenance, fluconazole performed poorly in comparison to other azoles. 3. ART We found one study, in which one out of seven participants in the 'early' arm and none of the three participants in the 'late' arm died.
AUTHORS' CONCLUSIONS: Liposomal amphotericin B appears to be a better choice compared to deoxycholate amphotericin B for treating PDH in people with HIV; and fluconazole performed poorly compared to other azoles. Other treatment choices for induction, maintenance, and when to start ART have no evidence, or very low certainty evidence. PDH needs prospective comparative trials to help inform clinical decisions.
进行性播散性组织胞浆菌病(PDH)是一种严重的真菌感染,影响着艾滋病病毒感染者。治疗该疾病的最佳方法尚不清楚。
我们评估了三个存在 equipoise 的领域的证据。1. 诱导治疗。比较脂质体两性霉素 B 初始治疗与其他抗真菌药物初始治疗的疗效和安全性。2. 维持治疗。比较 12 个月口服抗真菌药物维持治疗与较短疗程维持治疗的疗效和安全性。3. 抗逆转录病毒治疗(ART)。比较早期启动 ART 与延迟启动 ART 的结果。
我们检索了Cochrane传染病组专业注册库;Cochrane 中心对照试验注册库;MEDLINE(PubMed);Embase(Ovid);科学引文索引扩展版、会议论文引文索引 - 科学版和生物学文摘数据库(均来自科学网);世界卫生组织国际临床试验注册平台、ClinicalTrials.gov 和 ISRCTN 注册库,检索截止至2020年3月20日。
我们评估了评估脂质体两性霉素 B 和其他抗真菌药物用于诱导治疗的研究;评估抗真菌药物维持治疗疗程的研究;以及评估 ART 启动时机的研究。我们纳入了随机对照试验(RCT)、单臂试验、前瞻性队列研究和单臂队列研究。
两位综述作者评估了纳入资格和偏倚风险,提取了数据,并评估了证据的确定性。我们使用Cochrane“偏倚风险”工具评估随机研究中的偏倚风险,并使用ROBINS - I工具评估非随机研究中的偏倚风险。我们使用风险比(RRs)及95%置信区间(CI)总结二分法结局。
我们识别出17项个体研究。我们判定其中8项研究存在严重偏倚风险,并将其排除在分析之外。1. 诱导治疗 我们发现一项RCT,比较了脂质体两性霉素 B 和去氧胆酸盐两性霉素 B。与去氧胆酸盐两性霉素 B 相比,脂质体两性霉素 B 可能具有更高的临床成功率(RR 1.46,95% CI 1.01至2.11;1项研究,80名参与者;低确定性证据)。与去氧胆酸盐两性霉素 B 相比,脂质体两性霉素 B 的肾毒性发生率更低(RR 0.25,95% CI 0.09至0.67;1项研究,77名参与者;高确定性证据)。我们发现极低确定性证据可用于比较两性霉素 B 制剂与唑类药物用于诱导治疗的情况。2. 维持治疗 我们未找到符合条件的研究来比较少于12个月口服抗真菌药物维持治疗与12个月或更长时间维持治疗的情况。对于诱导治疗和维持治疗,与其他唑类药物相比,氟康唑的表现较差。3. ART 我们发现一项研究,“早期”组的7名参与者中有1人死亡,“晚期”组的3名参与者均未死亡。
与去氧胆酸盐两性霉素 B 相比,脂质体两性霉素 B 似乎是治疗艾滋病病毒感染者PDH的更好选择;与其他唑类药物相比,氟康唑的表现较差。关于诱导治疗、维持治疗以及何时开始ART的其他治疗选择尚无证据,或仅有极低确定性证据。PDH需要前瞻性比较试验来为临床决策提供依据。




