Department of Respiratory Medicine, University College London, London, UK
Centre for Medical Image Computing, University College London, London, UK.
Thorax. 2020 Aug;75(8):648-654. doi: 10.1136/thoraxjnl-2019-213865. Epub 2020 Apr 28.
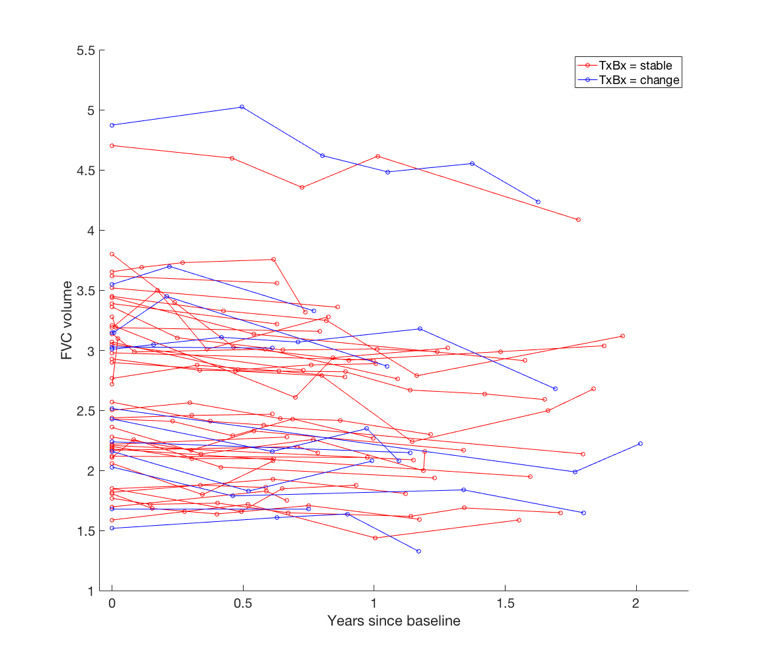
Patients with idiopathic pulmonary fibrosis (IPF) receiving antifibrotic medication and patients with non-IPF fibrosing lung disease often demonstrate rates of annualised forced vital capacity (FVC) decline within the range of measurement variation (5.0%-9.9%). We examined whether change in visual CT variables could help confirm whether marginal FVC declines represented genuine clinical deterioration rather than measurement noise.
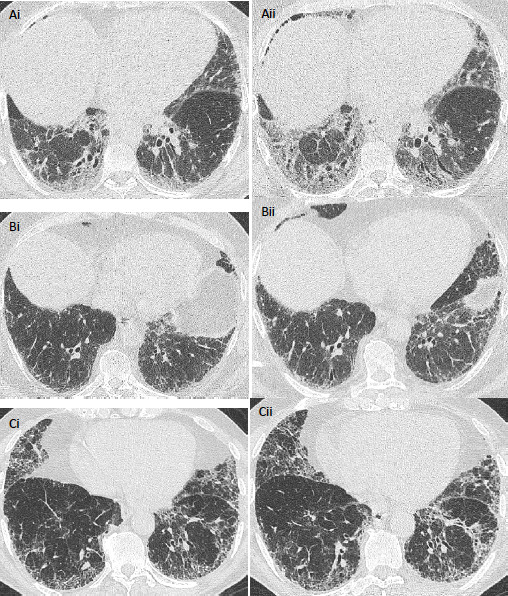
In two IPF cohorts (cohort 1: n=103, cohort 2: n=108), separate pairs of radiologists scored paired volumetric CTs (acquired between 6 and 24 months from baseline). Change in interstitial lung disease, honeycombing, reticulation, ground-glass opacity extents and traction bronchiectasis severity was evaluated using a 5-point scale, with mortality prediction analysed using univariable and multivariable Cox regression analyses. Both IPF populations were then combined to determine whether change in CT variables could predict mortality in patients with marginal FVC declines.
On univariate analysis, change in all CT variables except ground-glass opacity predicted mortality in both cohorts. On multivariate analysis adjusted for patient age, gender, antifibrotic use and baseline disease severity (diffusing capacity for carbon monoxide), change in traction bronchiectasis severity predicted mortality independent of FVC decline. Change in traction bronchiectasis severity demonstrated good interobserver agreement among both scorer pairs. Across all study patients with marginal FVC declines, change in traction bronchiectasis severity independently predicted mortality and identified more patients with deterioration than change in honeycombing extent.
Change in traction bronchiectasis severity is a measure of disease progression that could be used to help resolve the clinical importance of marginal FVC declines.
接受抗纤维化药物治疗的特发性肺纤维化 (IPF) 患者和非特发性肺纤维化性肺疾病患者的年度用力肺活量 (FVC) 下降率通常在测量变异性范围内 (5.0%-9.9%)。我们研究了视觉 CT 变量的变化是否有助于确认边缘性 FVC 下降是否代表真正的临床恶化,而不是测量噪声。
在两个 IPF 队列中(队列 1:n=103,队列 2:n=108),由两位独立的放射科医生对配对的容积 CT 进行评分(从基线开始的 6 至 24 个月之间采集)。使用 5 分制评估间质性肺病、蜂巢、网状、磨玻璃混浊程度和牵引性支气管扩张严重程度的变化,使用单变量和多变量 Cox 回归分析评估死亡率预测。然后将两个 IPF 人群合并,以确定 CT 变量的变化是否可以预测边缘性 FVC 下降患者的死亡率。
在单变量分析中,除磨玻璃混浊程度外,所有 CT 变量的变化均预测了两个队列的死亡率。在多变量分析中,调整了患者年龄、性别、抗纤维化药物使用和基线疾病严重程度(一氧化碳弥散量)后,牵引性支气管扩张严重程度的变化独立于 FVC 下降预测死亡率。在两个评分者对之间,牵引性支气管扩张严重程度的变化均具有良好的观察者间一致性。在所有研究中,边缘性 FVC 下降的患者中,牵引性支气管扩张严重程度的变化独立预测死亡率,并比蜂巢程度的变化识别出更多的病情恶化患者。
牵引性支气管扩张严重程度的变化是疾病进展的一种衡量标准,可以用于帮助解决边缘性 FVC 下降的临床重要性。