Research Department of Behavioural Science & Health, University College London and Head & Neck Cancer Centre, University College London Hospital, 250 Euston Road, Ground floor Central, London, NW1 2PQ, UK.
Division of Psychology & Language Sciences, University College London, London, UK.
BMC Cancer. 2020 Apr 29;20(1):360. doi: 10.1186/s12885-020-06877-3.
Dysphagia or difficulty in swallowing affects quality of life for most patients with head and neck cancer. SIP SMART - [Swallowing Intervention Package: Self-Monitoring, Assessment, Rehabilitation Training] aims to improve post-treatment swallowing outcomes through a targeted and tailored pre-treatment intervention. This feasibility study assessed 1) recruitment and retention, 2) patient acceptability of randomisation and participation, 3) patient adherence, and 4) sought to identify a suitable primary outcome for a definitive trial, including sample size estimation.
This two-arm parallel group non-blinded randomised feasibility trial took place within a head and neck centre at a teaching hospital in London, UK. Patients newly diagnosed with stage III/IV head and neck cancer were recruited and underwent 6-month follow-up. Patients were randomised to SIP-SMART or usual care via an online web-based system. SIP SMART comprised two 45-min consultations including a baseline clinical and instrumental swallowing assessment, relevant educational information, targeted swallowing exercises, and specific behaviour change strategies to increase exercise adherence. Usual care comprised a single session including a baseline clinical assessment and generic information about the likely impact of treatment on swallowing.
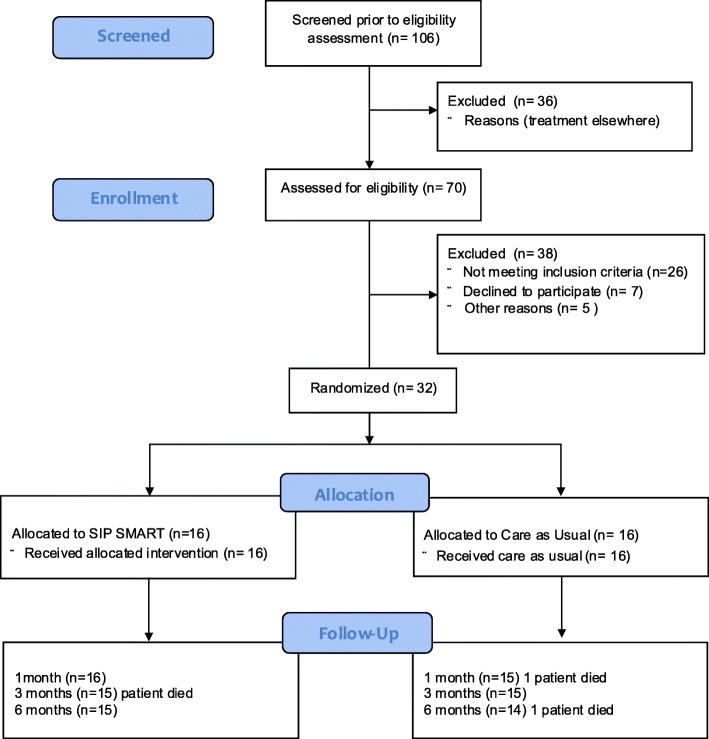
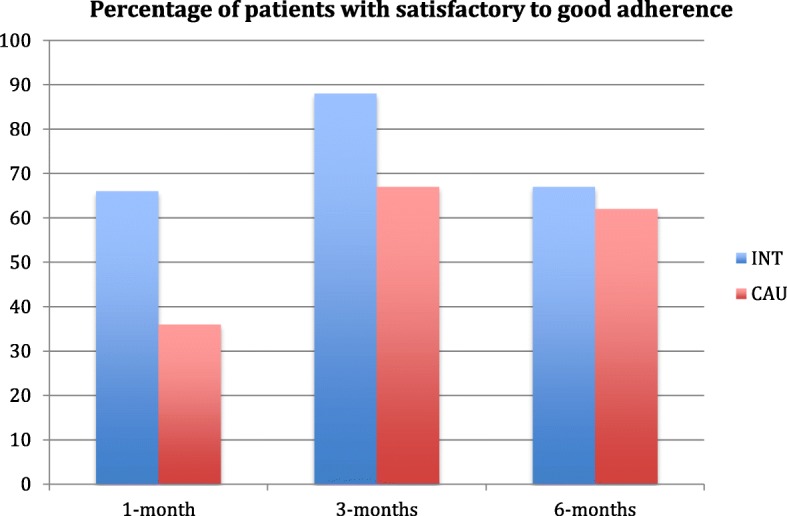
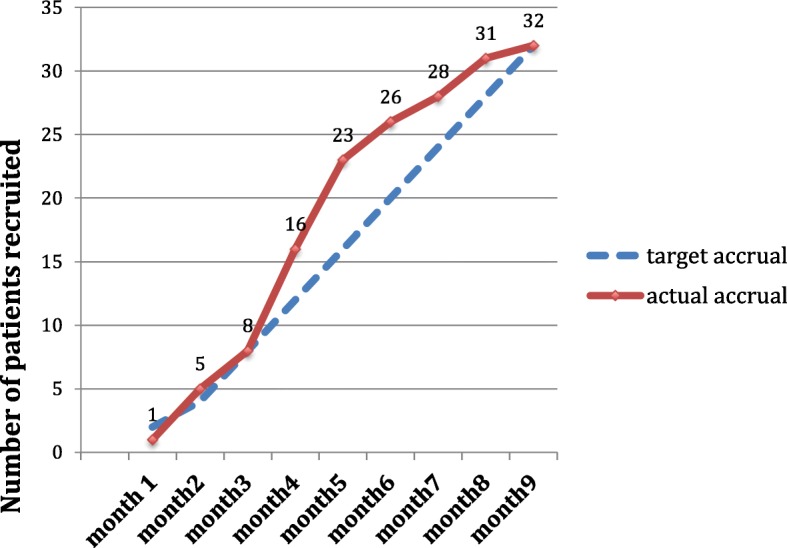
A total of 106 patients were identified at pre-screening, 70 were assessed for eligibility. Twenty-six patients did not meet eligibility criteria [0.37, 95% CI 0.27 to 0.49]. Five of 44 [0.11, 95% CI 0.05 to 0.24] eligible patients were not approached by researchers during clinic. Seven [0.18, 95% CI 0.08 to 0.33] of the 39 approached declined participation. Target recruitment (32 consented patients) was achieved within the timeframe. At 6-months 29/32 [0.91, 95% CI 0.76 to 0.97] patients remained in the trial. Acceptability of randomisation and participation in the intervention was favourable, and adherence to the exercises exceeded the pre-defined 35% minimum criterion. The MD Anderson Dysphagia Inventory swallow related quality of life measure was selected as the most suitable primary outcome for sample size estimation. No adverse effects arose from the intervention, or study participation.
A definitive trial of the SIP SMART intervention compared to usual care is feasible and can be undertaken with patients with head and neck cancer treated within the NHS.
ISRCTN40215425, registered retrospectively.
吞咽困难或吞咽困难会影响大多数头颈部癌症患者的生活质量。SIP SMART - [吞咽干预包:自我监测、评估、康复训练]旨在通过针对性和量身定制的治疗前干预来改善治疗后吞咽效果。这项可行性研究评估了 1) 招募和保留率,2) 患者对随机分组和参与的可接受性,3) 患者的依从性,并4) 试图为确证试验确定一个合适的主要结局,包括样本量估计。
这项两臂平行组非盲随机可行性试验在英国伦敦的一家教学医院的头颈部中心进行。新诊断为 III/IV 期头颈部癌症的患者被招募,并接受了 6 个月的随访。患者通过在线网络系统随机分配至 SIP-SMART 或常规护理。SIP SMART 包括两次 45 分钟的咨询,包括基线临床和仪器吞咽评估、相关教育信息、针对性吞咽练习以及特定的行为改变策略,以提高运动依从性。常规护理包括单次就诊,包括基线临床评估和关于治疗对吞咽影响的一般信息。
在预筛查时共确定了 106 名患者,其中 70 名符合入组标准。26 名患者不符合入选标准[0.37,95%置信区间 0.27 至 0.49]。在 44 名符合条件的患者中,有 5 名[0.11,95%置信区间 0.05 至 0.24]未被研究者在门诊接触到。在被接触的 39 名患者中,有 7 名[0.18,95%置信区间 0.08 至 0.33]拒绝参与。在规定的时间内达到了目标招募(32 名同意的患者)。在 6 个月时,32 名[0.91,95%置信区间 0.76 至 0.97]患者仍留在试验中。随机分组和参与干预的可接受性良好,对运动的依从性超过了预先设定的 35%最低标准。MD 安德森吞咽障碍量表吞咽相关生活质量测量被选为样本量估计的最合适的主要结局。干预或研究参与没有产生任何不良反应。
与常规护理相比,SIP SMART 干预的确证试验是可行的,可以在 NHS 治疗的头颈部癌症患者中进行。
ISRCTN40215425,回顾性注册。