Department of Cardiology and Angiology, Hannover Medical School, Carl-Neuberg-Str. 1, D-30659, Hannover, Germany.
Cardiovasc Drugs Ther. 2020 Aug;34(4):555-568. doi: 10.1007/s10557-020-06981-3.
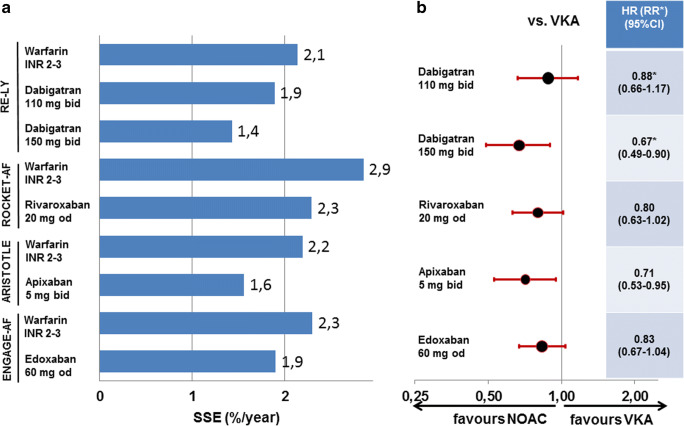
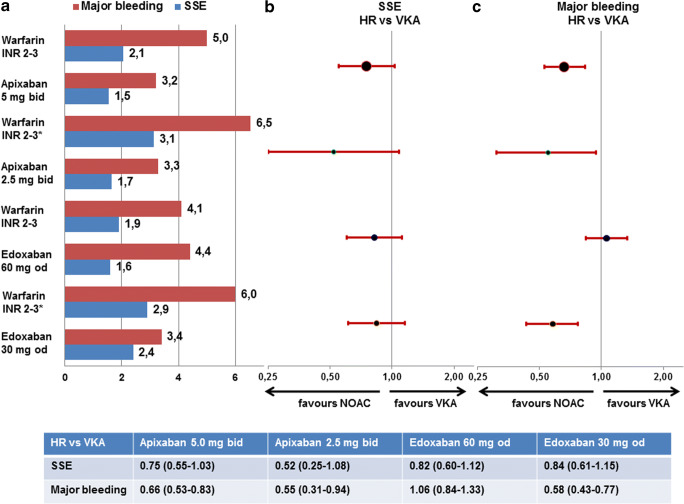
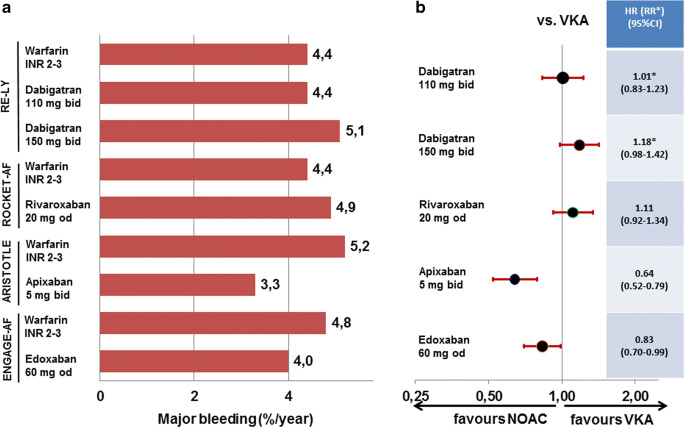
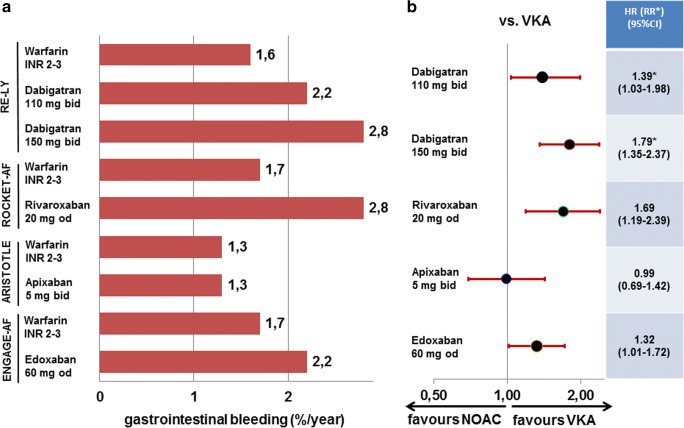
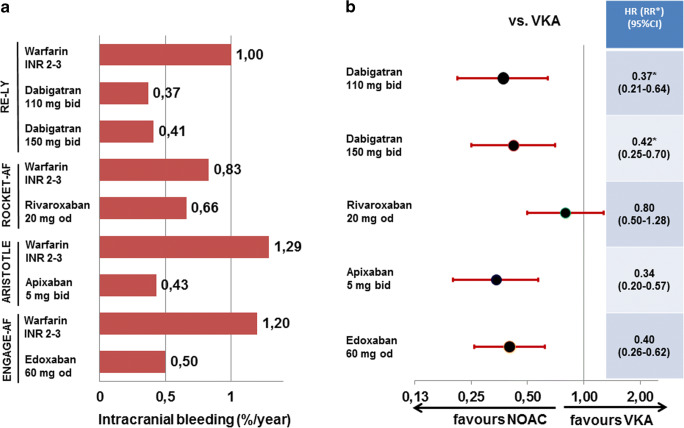
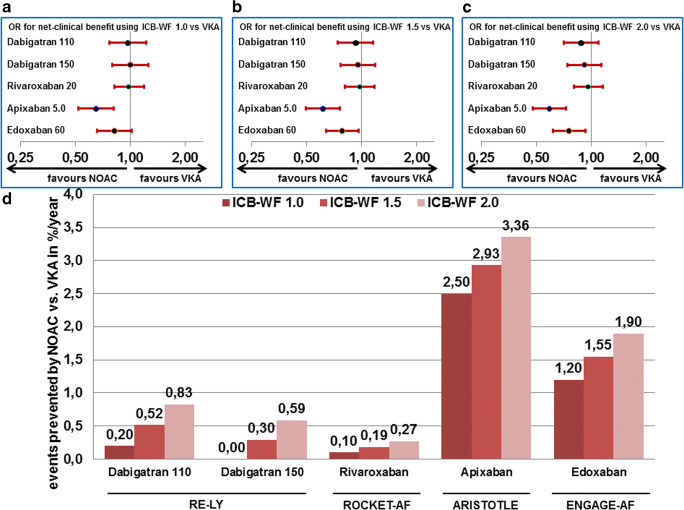
Ischaemic stroke and systemic embolism are the major potentially preventable complications of atrial fibrillation (AF) leading to severe morbidity and mortality. Anticoagulation using vitamin K antagonists (VKA) or non-vitamin K oral anticoagulants (NOACs) is mandatory for stroke prevention in AF. Following approval of the four NOACs dabigatran, rivaroxaban, apixaban, and edoxaban, the use of VKA is declining steadily. Increasing age with thresholds of 65 and 75 years is a strong risk factor when determining annual stroke risk in AF patients. Current recommendations such as the "2016 Guidelines for the management of atrial fibrillation" of the European Society of Cardiology and the "2019 AHA/ACC/HRS Focused Update" by the American College of Cardiology, the American Heart Association, and the Heart Rhythm Society strengthen the importance of anticoagulation and detection of bleeding risks, of which older age is an important one. While patients aged ≥ 75 years are usually underrepresented in randomised clinical trials, they represent almost 40% of the trial populations in the large NOAC approval studies. Therefore, a sufficient amount of data is available to assess the efficacy and safety for this patient cohort in that specific indication. In this article, the evidence for stroke prevention in AF using either VKA or NOACs is summarised with a special focus on efficacy compared to bleeding risk in patients aged ≥ 75 years. Specifically, we used a model of increased weighing of intracranial bleeding to illustrate the potential benefit of NOACs over VKA in the elderly population. In brief, there are at least two tested strategies with apixaban and edoxaban which even confer an additional clinical net benefit compared with VKA. Furthermore, elderly subgroups of trials for combined antithrombotic treatment following percutaneous coronary interventions in anticoagulated patients are analysed.
缺血性卒中和系统性栓塞是导致严重发病率和死亡率的房颤(AF)的主要潜在可预防并发症。维生素 K 拮抗剂(VKA)或非维生素 K 口服抗凝剂(NOAC)的抗凝治疗对于 AF 患者的卒中预防是强制性的。在批准了四种 NOAC 药物(达比加群、利伐沙班、阿哌沙班和依度沙班)后,VKA 的使用量稳步下降。年龄增长是 AF 患者确定年度卒中风险的一个强有力的危险因素,阈值为 65 岁和 75 岁。目前的指南建议,如欧洲心脏病学会的“2016 年房颤管理指南”和美国心脏病学会、美国心脏协会和心律学会的“2019 年 AHA/ACC/HRS 重点更新”,强调了抗凝和出血风险检测的重要性,其中年龄较大是一个重要因素。虽然≥75 岁的患者在随机临床试验中通常代表性不足,但他们在大型 NOAC 批准研究的试验人群中占近 40%。因此,有足够的数据可用于评估该特定适应证中该患者人群的疗效和安全性。在本文中,总结了使用 VKA 或 NOAC 预防 AF 卒中的证据,特别关注了在≥75 岁患者中与出血风险相比的疗效。具体来说,我们使用颅内出血风险加权增加的模型来说明与 VKA 相比,NOAC 在老年人群中的潜在获益。简而言之,与 VKA 相比,阿哌沙班和依度沙班至少有两种经过测试的策略可带来额外的临床净获益。此外,还分析了抗凝患者经皮冠状动脉介入治疗后联合抗血栓治疗的老年亚组试验。