Pulmonary Science and Critical Care Medicine, Denver Health Medical Center and University of Colorado, Anschutz Medical Campus, Denver, CO.
Pulmonary, Critical Care and Sleep Medicine, Ben Taub Hospital, Houston, TX.
Chest. 2020 Oct;158(4):1431-1445. doi: 10.1016/j.chest.2020.04.025. Epub 2020 Apr 27.
Fluid and vasopressor management in septic shock remains controversial. In this randomized controlled trial, we evaluated the efficacy of dynamic measures (stroke volume change during passive leg raise) to guide resuscitation and improve patient outcome.
Will resuscitation that is guided by dynamic assessments of fluid responsiveness in patients with septic shock improve patient outcomes?
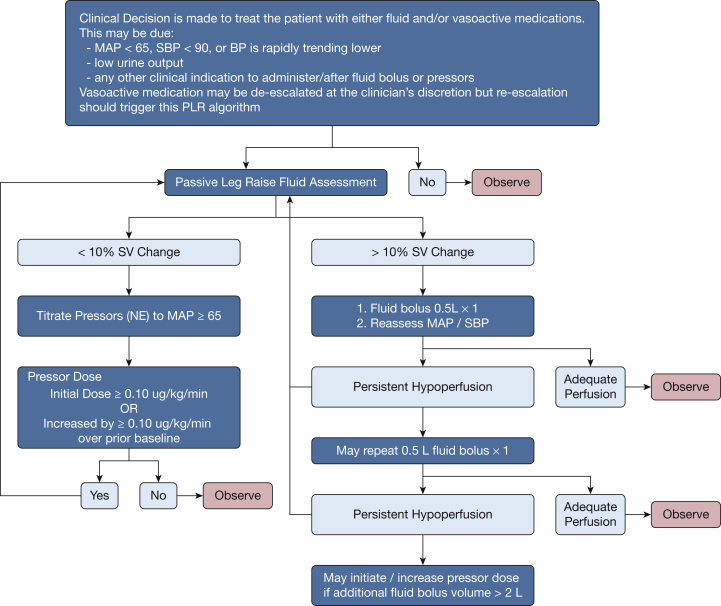
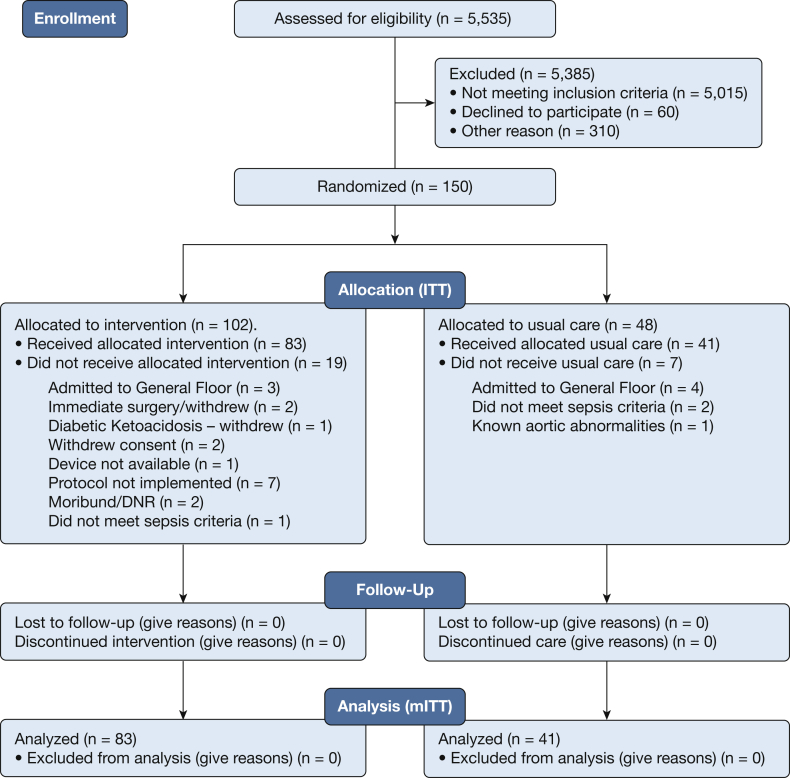
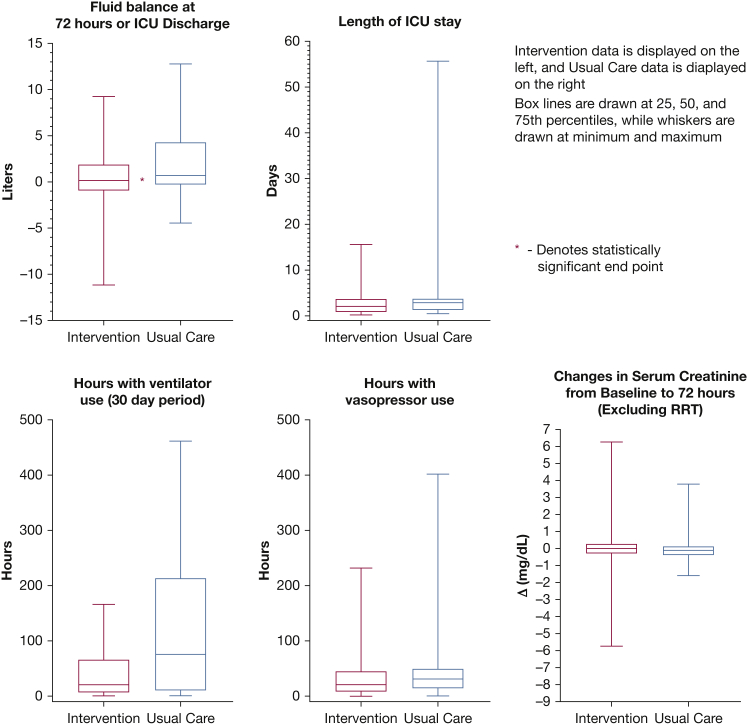
We conducted a prospective, multicenter, randomized clinical trial at 13 hospitals in the United States and United Kingdom. Patients presented to EDs with sepsis that was associated hypotension and anticipated ICU admission. Intervention arm patients were assessed for fluid responsiveness before clinically driven fluid bolus or increase in vasopressors occurred. The protocol included reassessment and therapy as indicated by the passive leg raise result. The control arm received usual care. The primary clinical outcome was positive fluid balance at 72 hours or ICU discharge, whichever occurred first.
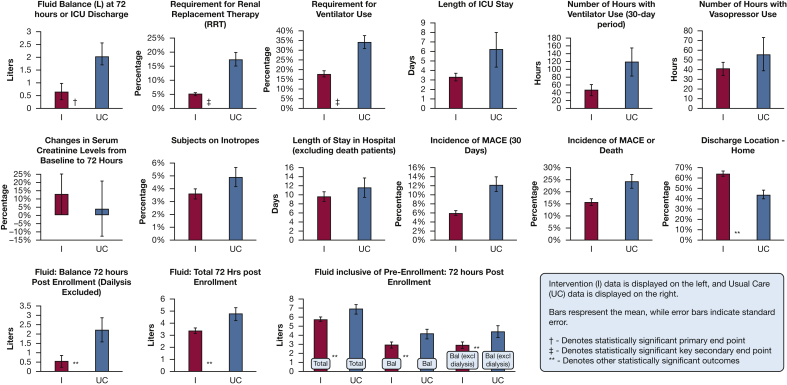
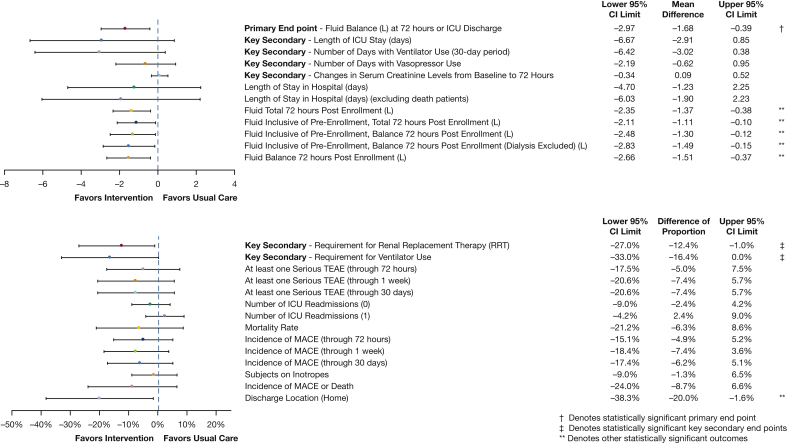
In modified intent-to-treat analysis that included 83 intervention and 41 usual care eligible patients, fluid balance at 72 hours or ICU discharge was significantly lower (-1.37 L favoring the intervention arm; 0.65 ± 2.85 L intervention arm vs 2.02 ± 3.44 L usual care arm; P = .021. Fewer patients required renal replacement therapy (5.1% vs 17.5%; P = .04) or mechanical ventilation (17.7% vs 34.1%; P = .04) in the intervention arm compared with usual care. In the all-randomized intent-to-treat population (102 intervention, 48 usual care), there were no significant differences in safety signals.
Physiologically informed fluid and vasopressor resuscitation with the use of the passive leg raise-induced stroke volume change to guide management of septic shock is safe and demonstrated lower net fluid balance and reductions in the risk of renal and respiratory failure. Dynamic assessments to guide fluid administration may improve outcomes for patients with septic shock compared with usual care.
NCT02837731.
脓毒性休克患者的液体和血管加压素管理仍存在争议。在这项随机对照试验中,我们评估了动态指标(被动抬腿期间的每搏量变化)指导复苏并改善患者结局的疗效。
通过对脓毒性休克患者液体反应性的动态评估进行复苏是否会改善患者结局?
我们在美国和英国的 13 家医院进行了一项前瞻性、多中心、随机临床试验。患者因败血症出现低血压并预计需要入住 ICU 而到急诊科就诊。干预组患者在进行临床驱动的液体冲击或血管加压剂增加之前,评估液体反应性。方案包括根据被动抬腿结果进行重新评估和治疗。对照组接受常规护理。主要临床结局为 72 小时或 ICU 出院时的正液体平衡,以先发生者为准。
在包括 83 名干预组和 41 名常规护理组合格患者的意向治疗分析中,72 小时或 ICU 出院时的液体平衡显著较低(有利于干预组,差值为-1.37L;0.65±2.85L 干预组 vs 2.02±3.44L 常规护理组;P=0.021)。与常规护理组相比,干预组需要肾脏替代治疗(5.1% vs 17.5%;P=0.04)或机械通气(17.7% vs 34.1%;P=0.04)的患者更少。在所有随机意向治疗人群(102 名干预组,48 名常规护理组)中,安全性信号无显著差异。
使用被动抬腿引起的每搏量变化指导脓毒性休克的液体和血管加压素复苏的生理导向液体和血管加压素复苏是安全的,并显示出更低的净液体平衡,降低了肾衰竭和呼吸衰竭的风险。与常规护理相比,使用动态评估来指导液体管理可能会改善脓毒性休克患者的结局。
NCT02837731。