Divisions of Maternal-Fetal Medicine, TriHealth-Good Samaritan Hospital, Cincinnati, OH.
Pulmonology and Critical Care Medicine, TriHealth-Good Samaritan Hospital, Cincinnati, OH.
Am J Obstet Gynecol MFM. 2020 Aug;2(3):100120. doi: 10.1016/j.ajogmf.2020.100120. Epub 2020 Apr 14.
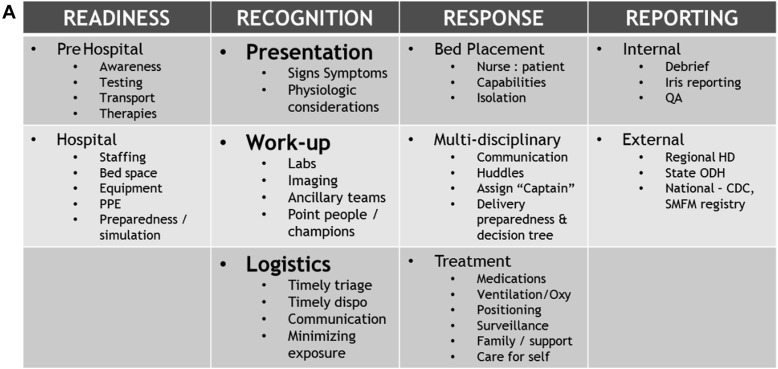
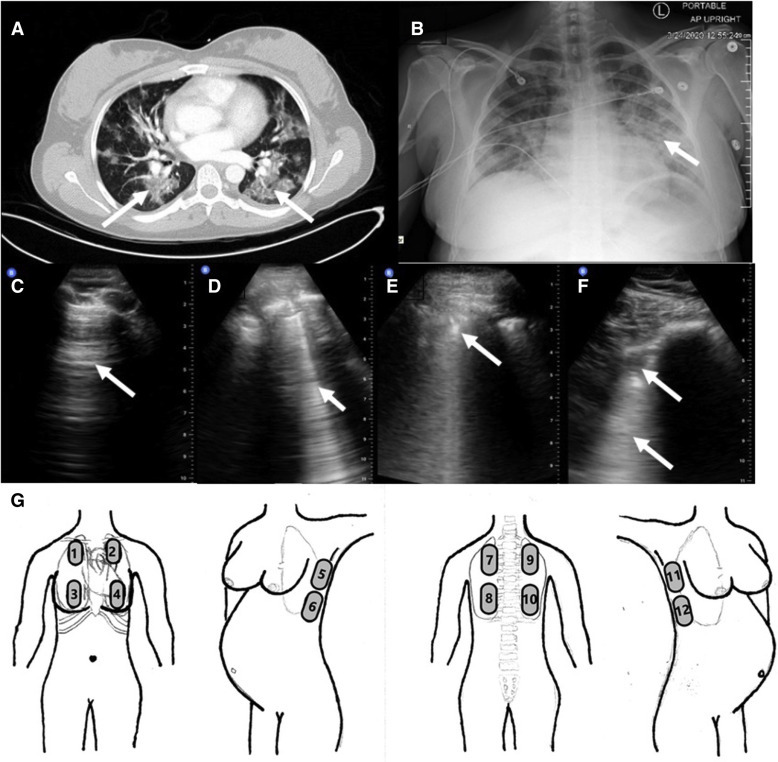
Since the emergence of a novel coronavirus (severe acute respiratory syndrome coronavirus 2) in Wuhan, China, at the end of December 2019, coronavirus disease 2019 has been associated with severe morbidity and mortality and has left world governments, healthcare systems, and providers caring for vulnerable populations, such as pregnant women, wrestling with the optimal management strategy. Unique physiologic and ethical considerations negate a one-size-fits-all approach when caring for critically ill pregnant women with coronavirus disease 2019, and few resources exist to guide the multidisciplinary team through decisions regarding optimal maternal-fetal surveillance, intensive care procedures, and delivery timing. We present a case of rapid clinical decompensation and development of severe acute respiratory distress syndrome in a woman at 31 weeks' gestation to highlight these unique considerations and present an algorithmic approach to the diagnosis and management of the disease.
自 2019 年 12 月底中国武汉出现新型冠状病毒(严重急性呼吸综合征冠状病毒 2)以来,2019 年冠状病毒病与严重发病率和死亡率相关,使世界各国政府、医疗保健系统和为弱势群体(如孕妇)提供护理的提供者都在努力制定最佳管理策略。在照顾患有 2019 年冠状病毒病的危重孕妇时,独特的生理和伦理考虑因素否定了一刀切的方法,而且几乎没有资源可指导多学科团队做出关于最佳母婴监测、重症监护程序和分娩时机的决策。我们报告了一例 31 周妊娠的妇女迅速临床恶化并发展为严重急性呼吸窘迫综合征的病例,以强调这些独特的考虑因素,并提出了一种用于诊断和管理该疾病的算法方法。