Department of Dermatology, University Hospital Essen, University of Duisburg-Essen, Essen, Germany.
Center of Clinical Epidemiology, Institute for Medical Informatics, Biometry and Epidemiology, University of Duisburg-Essen, Essen, Germany.
J Immunother Cancer. 2020 May;8(1). doi: 10.1136/jitc-2019-000395.
Immune checkpoint inhibition (ICI) is an essential treatment option in melanoma. Its outcome may be improved by a preceding radiation of metastases. This study aimed to investigate the impact of a preceding radiotherapy on the clinical outcome of ICI treatment.
This multicenter retrospective cohort study included patients who received anti-cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) or anti-programmed cell death protein 1 (PD-1) ICI with or without preceding radiotherapy for unresectable metastatic melanoma. ICI therapy outcome was measured as best overall response (BOR), progression-free (PFS) and overall survival (OS). Response and survival analyses were adjusted for confounders identified by directed acyclic graphs. Adjusted survival curves were calculated using inverse probability treatment weighting.
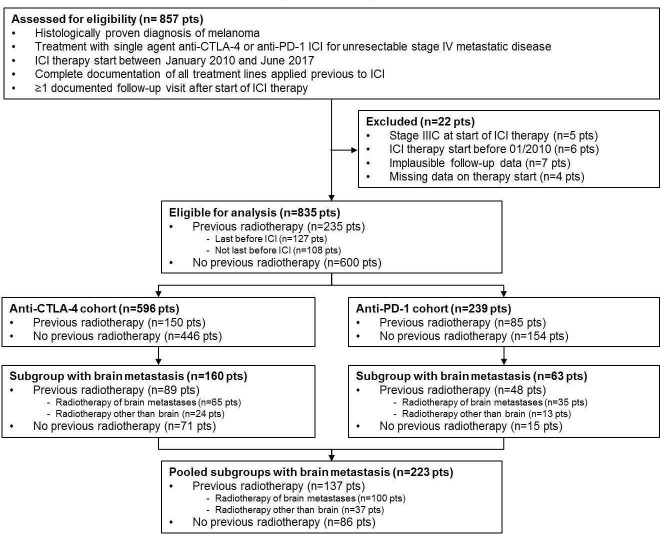
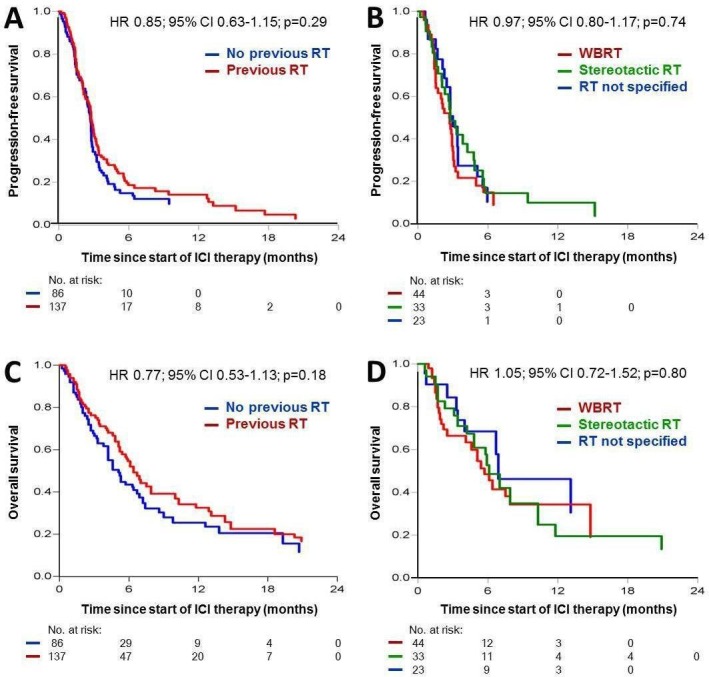
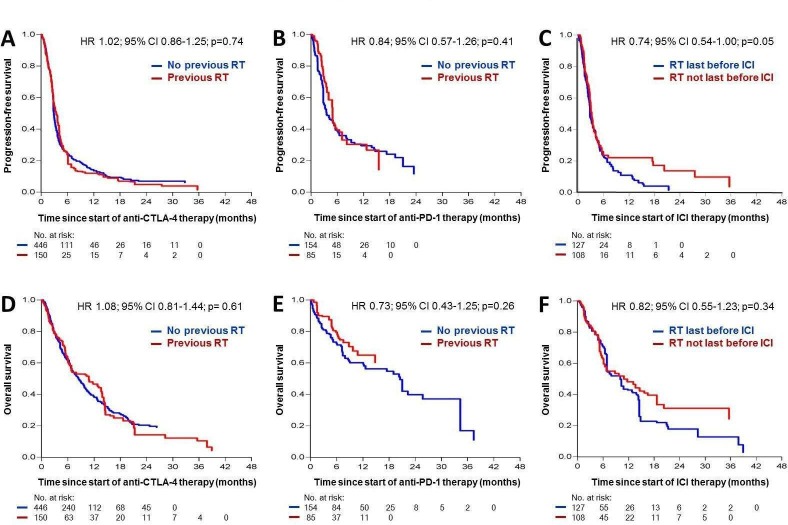
835 patients who received ICI (anti-CTLA-4, n=596; anti-PD-1, n=239) at 16 centers were analyzed, whereof 235 received a preceding radiotherapy of metastatic lesions in stage IV disease. The most frequent organ sites irradiated prior to ICI therapy were brain (51.1%), lymph nodes (17.9%) and bone (17.9%). After multivariable adjustment for confounders, no relevant differences in ICI therapy outcome were observed between cohorts with and without preceding radiotherapy. BOR was 8.7% vs 13.0% for anti-CTLA-4 (adjusted relative risk (RR)=1.47; 95% CI=0.81 to 2.65; p=0.20), and 16.5% vs 25.3% for anti-PD-1 (RR=0.93; 95% CI=0.49 to 1.77; p=0.82). Survival probabilities were similar for cohorts with and without preceding radiotherapy, for anti-CTLA-4 (PFS, adjusted HR=1.02, 95% CI=0.86 to 1.25, p=0.74; OS, HR=1.08, 95% CI=0.81 to 1.44, p=0.61) and for anti-PD-1 (PFS, HR=0.84, 95% CI=0.57 to 1.26, p=0.41; OS, HR=0.73, 95% CI=0.43 to 1.25, p=0.26). Patients who received radiation last before ICI (n=137) revealed no better survival than those who had one or more treatment lines between radiation and start of ICI (n=86). In 223 patients with brain metastases, we found no relevant survival differences on ICI with and without preceding radiotherapy.
This study detected no evidence for a relevant favorable impact of a preceding radiotherapy on anti-CTLA-4 or anti-PD-1 ICI treatment outcome in metastatic melanoma.
免疫检查点抑制(ICI)是黑色素瘤的重要治疗选择。其疗效可通过转移灶的先前放疗得到改善。本研究旨在探讨先前放疗对 ICI 治疗临床结局的影响。
这项多中心回顾性队列研究纳入了接受抗细胞毒性 T 淋巴细胞相关蛋白 4(CTLA-4)或抗程序性细胞死亡蛋白 1(PD-1)ICI 治疗的不可切除转移性黑色素瘤患者,这些患者接受了或未接受先前放疗。ICI 治疗的结局通过最佳总体缓解(BOR)、无进展生存期(PFS)和总生存期(OS)来衡量。通过有向无环图确定的混杂因素对反应和生存分析进行了调整。使用逆概率治疗加权法计算调整后的生存曲线。
在 16 个中心分析了 835 名接受 ICI(抗 CTLA-4,n=596;抗 PD-1,n=239)治疗的患者,其中 235 名患者在 IV 期疾病中接受了转移性病变的先前放疗。在接受 ICI 治疗前最常照射的器官部位是脑(51.1%)、淋巴结(17.9%)和骨骼(17.9%)。在多变量调整混杂因素后,先前放疗组和未放疗组之间在 ICI 治疗结局方面没有观察到明显差异。抗 CTLA-4 的 BOR 分别为 8.7%和 13.0%(调整后的相对风险(RR)=1.47;95%CI=0.81 至 2.65;p=0.20),抗 PD-1 的 BOR 分别为 16.5%和 25.3%(RR=0.93;95%CI=0.49 至 1.77;p=0.82)。先前放疗组和未放疗组的生存概率相似,抗 CTLA-4(PFS,调整 HR=1.02,95%CI=0.86 至 1.25,p=0.74;OS,HR=1.08,95%CI=0.81 至 1.44,p=0.61)和抗 PD-1(PFS,HR=0.84,95%CI=0.57 至 1.26,p=0.41;OS,HR=0.73,95%CI=0.43 至 1.25,p=0.26)。在 ICI 之前接受最后一次放疗的患者(n=137)的生存情况并不优于在放疗和 ICI 开始之间接受了一次或多次治疗的患者(n=86)。在 223 名有脑转移的患者中,我们发现放疗对 ICI 的生存影响无显著差异。
本研究未发现先前放疗对转移性黑色素瘤抗 CTLA-4 或抗 PD-1 ICI 治疗结局有明显的有利影响。