Care Delivery Research, Allina Health, 800 E 28th Street, MR 15521, Minneapolis, MN, USA.
Mental Health Clinic, Allina Health, 800 E 28th Street, Minneapolis, MN, USA.
Arch Womens Ment Health. 2021 Feb;24(1):133-144. doi: 10.1007/s00737-020-01035-x. Epub 2020 May 5.
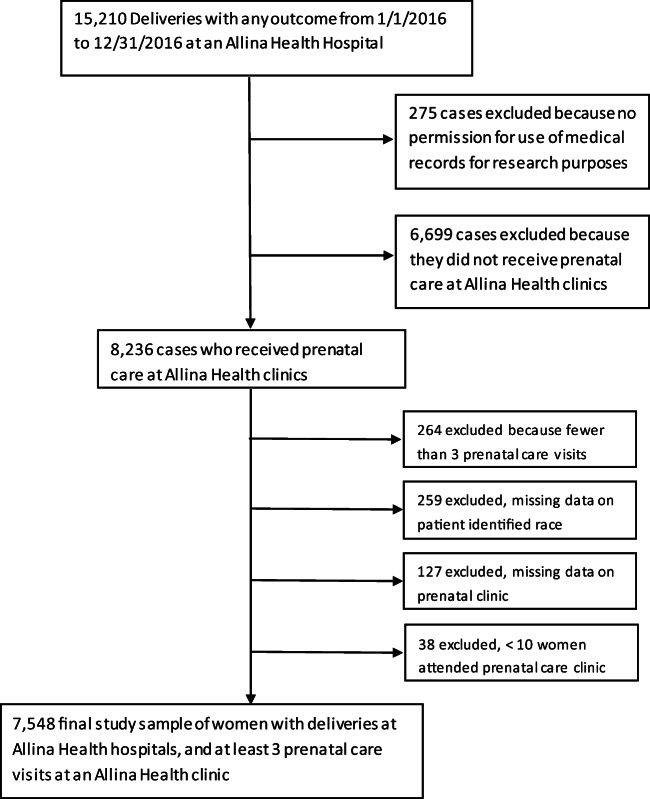
The purpose of this study was to assess the prevalence of prenatal and postpartum depression screening in a large health system and to identify covariates for screening, with a specific focus in understanding disparities in practice. A retrospective cohort of women with deliveries in 2016 was created using electronic health records. Primary outcomes were depression screening during pregnancy and the first 3 months postpartum. Generalized linear mixed models with women nested within clinic were used to determine the effect of maternal and clinical characteristics on depression screening. The sample included 7548 women who received prenatal care at 35 clinics and delivered at 10 hospitals. The postpartum sample included 7059 women who returned within 3 months for a postpartum visit. Of those, 65.1% were screened for depression during pregnancy, and 64.4% were screened postpartum. Clinic site was the strongest predictor of screening, accounting for 23-30% of the variability in screening prevalence. There were no disparities identified with regard to prenatal screening. However, several disparities were identified for postpartum screening. After adjusting for clinic, women who were African American, Asian, and otherwise non-white (Native American, multi-racial) were less likely to be screened postpartum than white women (AOR (CI)'s 0.81 (0.65, 1.01), 0.64 (0.53, 0.77), and 0.44 (0.21, 0.96), respectively). Women insured by Medicaid/Medicare, a proxy for low-income, were less likely to be screened postpartum than women who were privately insured (AOR (CI) 0.78 (0.68, 0.89)). National guidelines support universal depression screening of pregnant and postpartum women. The current study found opportunities for improvement in order to achieve universal screening and to deliver equitable care.
本研究旨在评估大型医疗系统中产前和产后抑郁症筛查的流行情况,并确定筛查的协变量,特别关注了解实践中的差异。使用电子健康记录创建了一个 2016 年分娩的妇女回顾性队列。主要结局是在怀孕期间和产后 3 个月进行抑郁症筛查。使用嵌套在诊所内的妇女的广义线性混合模型来确定母婴特征对抑郁症筛查的影响。该样本包括在 35 个诊所接受产前护理并在 10 家医院分娩的 7548 名妇女。产后样本包括在 3 个月内返回进行产后访视的 7059 名妇女。其中,65.1%在怀孕期间接受了抑郁症筛查,64.4%在产后接受了筛查。诊所地点是筛查率差异的最强预测因素,占筛查率差异的 23-30%。在产前筛查方面没有发现差异。然而,产后筛查方面存在一些差异。在调整诊所因素后,非裔美国人、亚裔和其他非白人(美洲原住民、多种族)妇女产后接受筛查的可能性低于白人妇女(AOR(CI)分别为 0.81(0.65,1.01)、0.64(0.53,0.77)和 0.44(0.21,0.96))。医疗保险/医疗补助(Medicaid/Medicare)承保的妇女,这是低收入的一个代表,产后接受筛查的可能性低于私人保险的妇女(AOR(CI)0.78(0.68,0.89))。国家指南支持对孕妇和产后妇女进行普遍的抑郁症筛查。本研究发现,为了实现普遍筛查和提供公平的护理,仍有改进的空间。