Mvundura Mercy, Di Giorgio Laura, Vodicka Elisabeth, Kindoli Robert, Zulu Chipo
Medical Devices and Health Technologies Program, PATH, Seattle, USA.
Center for Vaccine Innovation and Access, PATH, Seattle, USA.
Pan Afr Med J. 2020 Feb 12;35(Suppl 1):11. doi: 10.11604/pamj.supp.2020.35.1.17804. eCollection 2020.
Poor data quality and use have been identified as key challenges that negatively impact immunization programs in low- and middle-income countries (LMICs). In addition, many LMICs have a shortage of health personnel, and staff available have demanding workloads across several health programs. In order to address these challenges, the Better Immunization Data (BID) Initiative introduced a comprehensive suite of interventions, including an electronic immunization registry aimed at improving the quality, reliability, and use of immunization data in Arusha Region, Tanzania, and Southern Province of Zambia. The objective of this study was to assess the incremental costs of implementing the BID interventions in immunization programs in these two countries.
We conducted a micro-costing study to estimate the economic costs of service delivery and logistics for the immunization programs with and without the BID interventions in a sample of health facilities and district program offices in each country. Structured questionnaires were used to interview immunization program staff at baseline and post-intervention to assess annual resource utilization and costs. Cost outcomes were reported as annual cost per facility, cost per district and changes in resource costs due to the BID interventions (i.e., costs associated with health worker time, start-up costs, etc.). Sub-group analyses were conducted by health facility to assess variation in costs by volume served and location (rural versus urban). One-way sensitivity analyses were conducted to identify influential parameters. Costs were reported in 2017 US dollars.
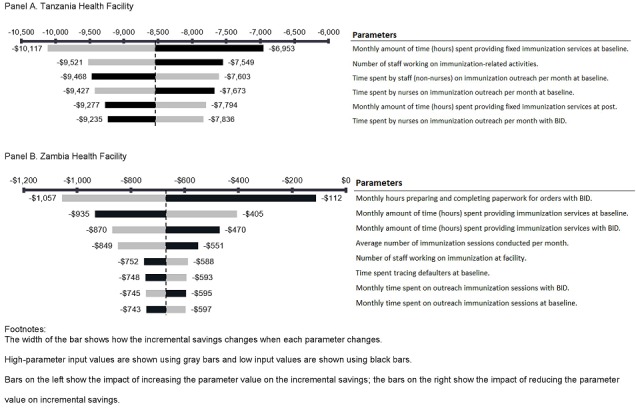
In Tanzania, the average annual reduction in resource costs was estimated at US$10,236 (95% confidence interval: $7,606-$14,123) per health facility, while the average annual reduction in resource costs per district was estimated at $6,542. In Zambia, reductions in resource costs were modest at an estimated annual average of $628 (95% confidence interval: $209-$1,467) per health facility and $236 per district. Resource cost reductions were mainly attributable to reductions in time required for immunization service delivery and reporting. One-way sensitivity analyses identified key cost drivers, all related to reductions in health worker time.
The introduction of electronic immunization registries and stock management systems through the BID Initiative was estimated to result in potential time savings in both countries. Health worker time was the area most impacted by the interventions, suggesting that time savings gained could be utilized for patient care. Information generated through this work provides evidence to inform stakeholder decision-making for scale-up of the BID interventions in Tanzania and Zambia and to inform other Low-to-Middle-Income Countries (LMICs) interested in similar interventions.
数据质量差及使用不当已被确定为对低收入和中等收入国家(LMICs)的免疫规划产生负面影响的关键挑战。此外,许多低收入和中等收入国家卫生人员短缺,现有工作人员在多个卫生项目中承担着繁重的工作量。为应对这些挑战,更好免疫数据(BID)倡议引入了一套全面的干预措施,包括一个电子免疫登记系统,旨在提高坦桑尼亚阿鲁沙地区和赞比亚南部省份免疫数据的质量、可靠性及利用率。本研究的目的是评估在这两个国家的免疫规划中实施BID干预措施的增量成本。
我们开展了一项微观成本核算研究,以估计在每个国家的一组卫生设施和地区项目办公室中,有和没有BID干预措施的免疫规划的服务提供和物流的经济成本。使用结构化问卷在基线和干预后对免疫规划工作人员进行访谈,以评估年度资源利用情况和成本。成本结果报告为每个设施的年度成本、每个地区的成本以及由于BID干预措施导致的资源成本变化(即与卫生工作者时间、启动成本等相关的成本)。按卫生设施进行亚组分析,以评估按服务量和地点(农村与城市)划分的成本差异。进行单向敏感性分析以确定有影响的参数。成本以2017年美元报告。
在坦桑尼亚,每个卫生设施的资源成本估计平均每年减少10,236美元(95%置信区间:7,606美元至14,123美元),而每个地区的资源成本估计平均每年减少6,542美元。在赞比亚,资源成本的减少幅度较小,估计每个卫生设施平均每年减少628美元(95%置信区间:209美元至1,467美元),每个地区减少236美元。资源成本的减少主要归因于免疫服务提供和报告所需时间的减少。单向敏感性分析确定了关键成本驱动因素,均与卫生工作者时间的减少有关。
通过BID倡议引入电子免疫登记系统和库存管理系统估计在这两个国家都能节省潜在时间。卫生工作者时间是受干预影响最大的领域,这表明节省的时间可用于患者护理。通过这项工作产生的信息为利益相关者在坦桑尼亚和赞比亚扩大BID干预措施的决策提供了依据,并为对类似干预措施感兴趣的其他低收入和中等收入国家提供了参考。