Wekesah Frederick M, Mutua Martin K, Boateng Daniel, Grobbee Diederick E, Asiki Gershim, Kyobutungi Catherine K, Klipstein-Grobusch Kerstin
African Population and Health Research Center, Nairobi, Kenya.
Julius Global Health, Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht University, the Netherlands.
Int J Cardiol Heart Vasc. 2020 Apr 28;28:100521. doi: 10.1016/j.ijcha.2020.100521. eCollection 2020 Jun.
Cardiovascular diseases (CVD) cause 18 million deaths annually. Low- and middle-income countries (LMICs) account for 80% of the CVD burden, and the burden is expected to grow in the region in the coming years. Screening for and identification of individuals at high risk for CVD in primary care settings can be accomplished using available CVD risk scores. However, few of these scores have been validated/recalibrated for use in sub-Saharan Africa (SSA).
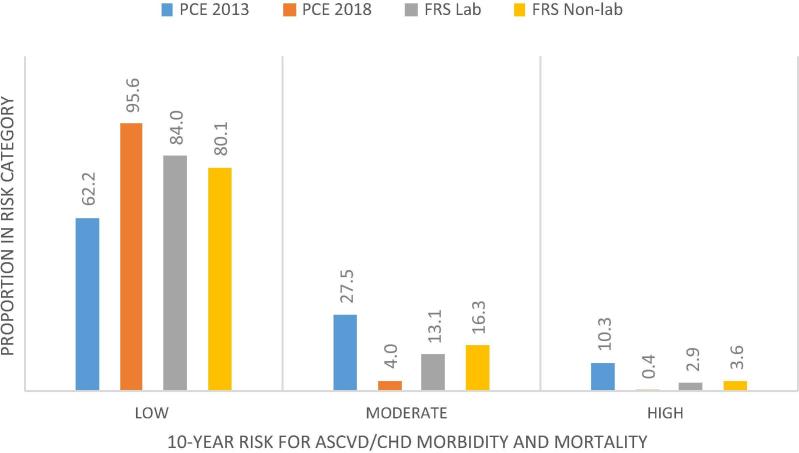
Pooled cohort equations (PCE) and Framingham risk scores for 10-year CVD risk were applied on 1960 men and women aged 40 years and older from the AWI-Gen (Africa, Wits-INDEPTH Partnership for GENomic studies) study 2015. Low, moderate/intermediate or high CVD risk classifications correspond to <10%, 10-20% and >20% chance of developing CVD in 10 years respectively. Agreement between the risk scores was assessed using kappa and correlation coefficients.
High CVD risk was 10.3% in PCE 2013, 0.4% in PCE 2018, 2.9% in Framingham and 3.6% in Framingham non-laboratory scores. Conversely, low CVD risk was 62.2% in PCE 2013 and 95.6% in PCE 2018, 84.0% and 80.1% in Framingham and Framingham non-laboratory scores, respectively. A moderate agreement existed between the Framingham functions (kappa = 0.64, 95% CI 0.59-0.68, correlation, r = 0.711). There was no agreement between the PCE 2013 and 2018 functions (kappa = 0.05, 95% CI 0.04-0.06).
Newer cohort-based data is necessary to validate and recalibrate existing CVD risk scores in order to develop appropriate functions for use in SSA.
心血管疾病(CVD)每年导致1800万人死亡。低收入和中等收入国家(LMICs)承担了80%的心血管疾病负担,预计未来几年该地区的负担还将增加。在初级保健机构中,使用现有的心血管疾病风险评分可以筛查和识别心血管疾病高危个体。然而,这些评分中很少有经过验证/重新校准可用于撒哈拉以南非洲(SSA)地区的。
对2015年AWI-Gen(非洲,威特沃特斯兰德大学深度基因组研究合作伙伴关系)研究中1960名40岁及以上的男性和女性应用了10年心血管疾病风险的合并队列方程(PCE)和弗雷明汉风险评分。低、中/中等或高心血管疾病风险分类分别对应10年内发生心血管疾病的概率<10%、10 - 20%和>20%。使用kappa系数和相关系数评估风险评分之间的一致性。
2013年PCE中高心血管疾病风险为10.3%,2018年PCE中为0.4%,弗雷明汉评分中为2.9%,弗雷明汉非实验室评分中为3.6%。相反,2013年PCE中低心血管疾病风险为62.2%,2018年PCE中为95.6%,弗雷明汉评分和弗雷明汉非实验室评分中分别为84.0%和80.1%。弗雷明汉函数之间存在中等程度的一致性(kappa = 0.64,95%CI 0.59 - 0.68,相关性,r = 0.711)。2013年和2018年PCE函数之间不存在一致性(kappa = 0.05,95%CI 0.04 - 0.06)。
需要更新的基于队列的数据来验证和重新校准现有的心血管疾病风险评分,以便开发适用于撒哈拉以南非洲地区的函数。