Ichioka Urological Clinic, Kyoto, Japan.
Department of Urology, Kyoto University Graduate School of Medicine, Kyoto, Japan.
Andrology. 2020 Sep;8(5):1214-1221. doi: 10.1111/andr.12812. Epub 2020 May 18.
Microdissection testicular sperm extraction (microTESE) is considered the gold standard method of sperm retrieval from patients with non-obstructive azoospermia (NOA). For careful and thorough examination of seminiferous tubules during microTESE, maximizing surface area of the testicles which we are able to search is essential.
To develop a systematic procedure for microTESE to maximize surface area and to achieve high sperm retrieval rate (SRR) in microTESE.
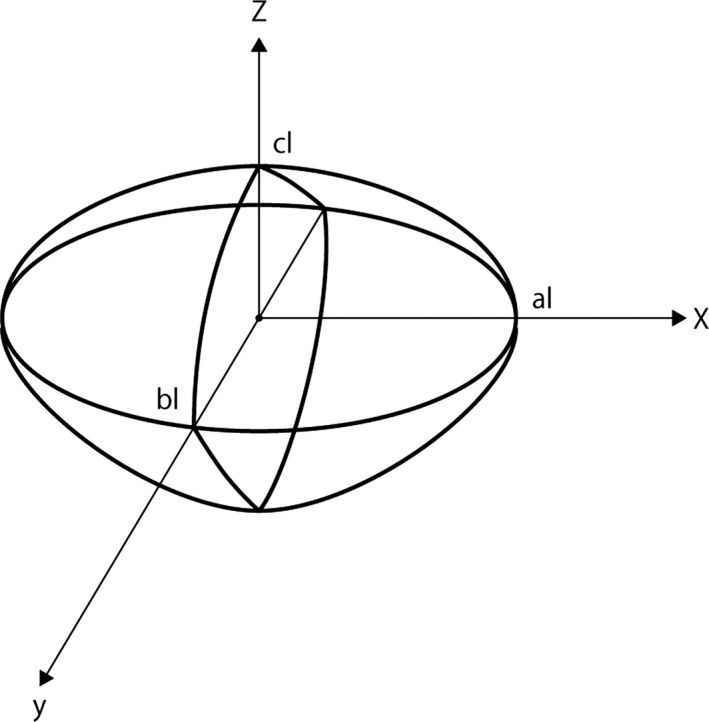
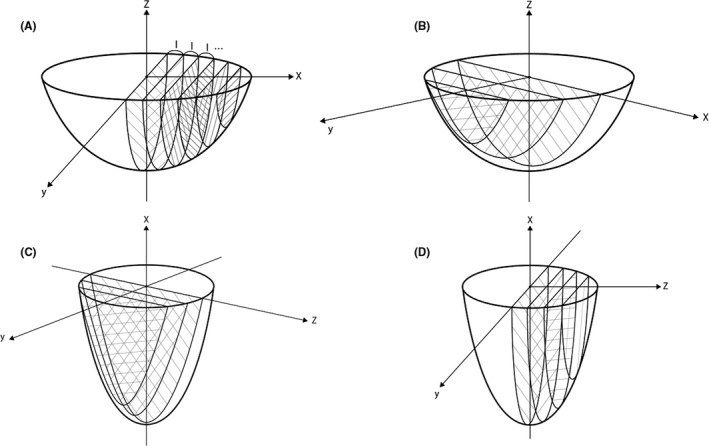
We simulated microTESE using three-dimensional (3D) simulation model and analyzed mathematically the sum of the surface area in various methods. The best method obtained from this simulation model was applied to 102 patients with NOA from 2014 to 2018. These new clinical results were compared with those of 56 patients who underwent a previous method of microTESE from 2011 to 2014.
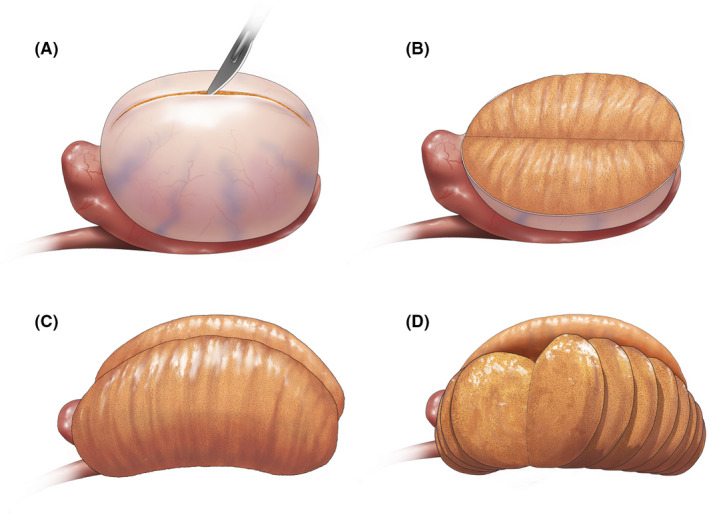
The mathematical 3D simulation model of microTESE indicated that a longitudinal incision on the tunica albuginea and following transverse slicing incisions of testicular parenchyma maximized the surface area coverage. Forty-six (45%) out of 102 patients who underwent microTESE with the new method had successful retrieval of testicular spermatozoa compared with 16 (29%) of 56 patients with the previous method of microTESE (P = .04).
Transverse resections of parenchyma in our method run parallel to the courses of intratesticular arteries and do not interfere with the blood supply. The small amount of extracted seminiferous tubules was equivalent to that of the previous method, and no patients exhibited post-operative symptoms of androgen deficiency in our study. As for post-operative pain, our new method was comparable with the previous method. Although our study needs a longer follow-up, there will be limited effects on testicular functions.
Longitudinal incision on the tunica albuginea and following transverse slicing incisions in the testicular parenchyma maximized the surface area and improved the SRR of microTESE.
显微睾丸精子提取术(microTESE)被认为是从非梗阻性无精子症(NOA)患者中获取精子的金标准方法。为了在 microTESE 过程中对生精小管进行仔细和彻底的检查,最大限度地增加我们能够搜索的睾丸表面积至关重要。
制定一种系统的 microTESE 程序,以最大限度地增加表面积,并实现 microTESE 中的高精子回收率(SRR)。
我们使用三维(3D)模拟模型模拟 microTESE,并对各种方法的表面积总和进行数学分析。从该模拟模型中获得的最佳方法应用于 2014 年至 2018 年的 102 名 NOA 患者。这些新的临床结果与 2011 年至 2014 年接受先前 microTESE 方法的 56 名患者的结果进行了比较。
microTESE 的数学 3D 模拟模型表明,在睾丸白膜上进行纵向切口,然后进行睾丸实质的横向切片切口,可最大限度地增加表面积覆盖范围。与先前的 microTESE 方法相比,采用新方法的 102 名患者中有 46 名(45%)成功获取睾丸精子,而采用先前方法的 56 名患者中只有 16 名(29%)(P = 0.04)。
我们的方法中的实质横向切除术与睾丸内动脉的走向平行,不会干扰血液供应。提取的生精小管数量与先前的方法相当,而且在我们的研究中没有患者出现雄激素缺乏的术后症状。至于术后疼痛,我们的新方法与先前的方法相当。虽然我们的研究需要更长的随访,但对睾丸功能的影响有限。
在睾丸白膜上进行纵向切口,然后在睾丸实质中进行横向切片切口可最大限度地增加表面积,并提高 microTESE 的 SRR。