Department of Diabetes, School of Life Course Sciences, King's College London, London, UK; Bariatric and Metabolic Surgery, King's College Hospital, London, UK.
Center for the treatment of Obesity and Diabetes, Oswaldo Cruz German Hospital, Sao Paulo, Brazil.
Lancet Diabetes Endocrinol. 2020 Jul;8(7):640-648. doi: 10.1016/S2213-8587(20)30157-1. Epub 2020 May 7.
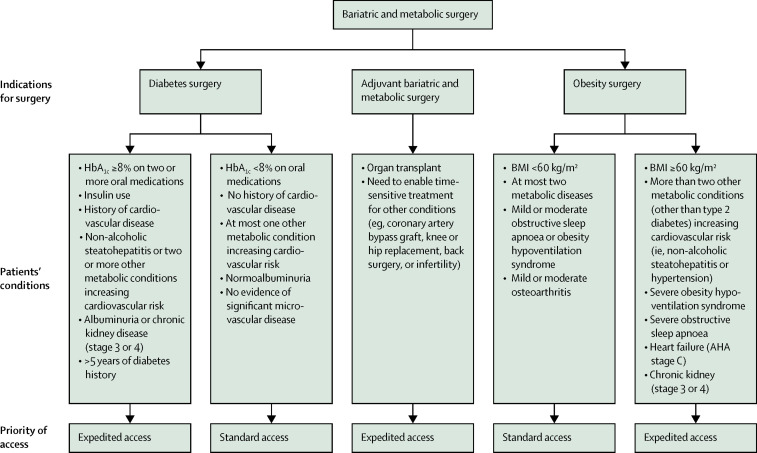
The coronavirus disease 2019 pandemic is wreaking havoc on society, especially health-care systems, including disrupting bariatric and metabolic surgery. The current limitations on accessibility to non-urgent care undermine postoperative monitoring of patients who have undergone such operations. Furthermore, like most elective surgery, new bariatric and metabolic procedures are being postponed worldwide during the pandemic. When the outbreak abates, a backlog of people seeking these operations will exist. Hence, surgical candidates face prolonged delays of beneficial treatment. Because of the progressive nature of obesity and diabetes, delaying surgery increases risks for morbidity and mortality, thus requiring strategies to mitigate harm. The risk of harm, however, varies among patients, depending on the type and severity of their comorbidities. A triaging strategy is therefore needed. The traditional weight-centric patient-selection criteria do not favour cases based on actual clinical needs. In this Personal View, experts from the Diabetes Surgery Summit consensus conference series provide guidance for the management of patients while surgery is delayed and for postoperative surveillance. We also offer a strategy to prioritise bariatric and metabolic surgery candidates on the basis of the diseases that are most likely to be ameliorated postoperatively. Although our system will be particularly germane in the immediate future, it also provides a framework for long-term clinically meaningful prioritisation.
2019 年冠状病毒病大流行正在给社会带来严重破坏,尤其是医疗保健系统,包括扰乱减重和代谢手术。目前对非紧急护理的获取限制,破坏了接受此类手术患者的术后监测。此外,与大多数择期手术一样,新的减重和代谢手术在全球大流行期间都被推迟。疫情缓解后,将有一大批人寻求这些手术。因此,手术候选人将面临治疗的长期延迟。由于肥胖和糖尿病的进展性质,延迟手术会增加发病率和死亡率的风险,因此需要采取策略来减轻伤害。然而,伤害的风险因患者而异,取决于其合并症的类型和严重程度。因此需要一种分诊策略。传统的以体重为中心的患者选择标准并不利于根据实际临床需求选择病例。在这篇个人观点中,来自糖尿病手术峰会共识会议系列的专家为手术延迟期间的患者管理和术后监测提供了指导。我们还提供了一种基于术后最有可能改善的疾病对减重和代谢手术候选人进行优先排序的策略。尽管我们的系统在不久的将来特别相关,但它也为长期有临床意义的优先级排序提供了框架。